
The American Academy of Dermatology has presented updated recommendations for the management of atopic dermatitis in patients under 18 years of age. The wide prevalence of this pathology in childhood and its chronic, relapsing nature make the selection of an effective treatment scheme a priority.
The guideline defines safety norms and dosing specifics in the pediatric treatment process in detail. Relying on evidence-based medicine, this approach ensures the establishment of a unified standard of therapy and the improvement of patients’ daily lives.
The Essence, Goals, and Challenges of Atopic Dermatitis Management
Atopic dermatitis is a common chronic inflammatory pathology in pediatric practice. In its management, primary attention is devoted to the suppression of the inflammatory process and acute itching, which represents a particular challenge in childhood. Since the disease manifests with periodic flares, the goal of medical intervention is symptomatic relief and the implementation of safe therapeutic approaches. Ultimately, effective management is determined by the improvement of the daily existence of patients and caregivers and an optimal balance of risks.
A wide spectrum of medicinal and non-medicinal means is used to treat the disease. However, conducting research in the pediatric sector is significantly hindered by ethical barriers, small samples, and methodological difficulties. It is this deficit of evidence that determines the use of preparations off-label, based on clinical experience. Although official guidelines rely on age restrictions established by the FDA, in practical medicine, effective therapy is often implemented in younger age groups as well.
Scope of the Guideline
A multidisciplinary team worked on the development of the document, which determined priority issues and the quality of evidence using the GRADE methodology from the initial stage of research. The guideline focuses on those patients under 18 years of age in whom atopic dermatitis of any severity is confirmed. Although the recommendations are universal for all types of medical institutions, they do not apply to immunocompromised individuals and patients with other concomitant skin pathologies.
The effectiveness of therapeutic interventions, including local, systemic, and photochemical therapy, was evaluated exclusively on the basis of randomized controlled trials (RCTs). During the process, the group relied on existing high-quality reviews, though in individual cases, a new (de novo) analysis was also conducted. The entire recommendation framework was defined by three fundamental questions concerning the safety and effectiveness of various types of therapy.
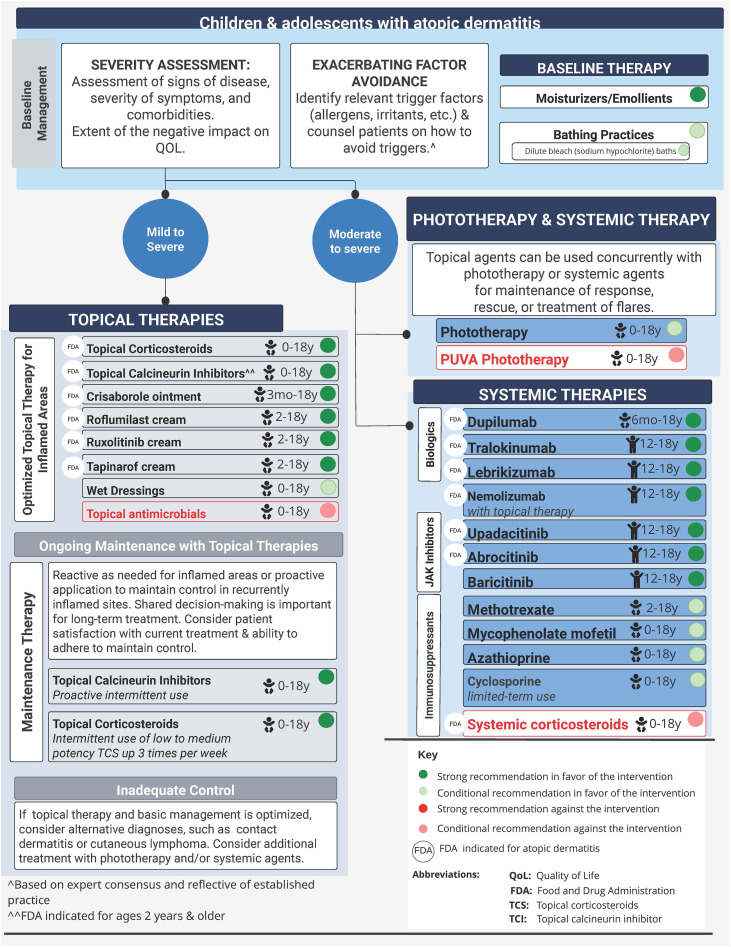
Over-the-Counter Local Therapy
Solid evidence from nine randomized trials assigns the highest quality recommendation to the use of moisturizers. Analysis of data from 1,260 pediatric patients showed that these means significantly reduce the Eczema Area and Severity Index (EASI), the Scoring Atopic Dermatitis scale (SCORAD), and total symptomatic scores.
Clinical observation (IGA) confirmed that with this therapeutic approach, the probability of complete or almost complete skin clearance (score of 0/1) increases significantly. At the same time, the treatment is distinguished by high safety—serious side effects are rare, and the rate of therapy discontinuation due to side effects does not exceed the data of the control group.
Despite this high therapeutic profile, the combined use of moisturizers and topical corticosteroids (TCS) for three weeks does not reveal additional clinical advantage compared to treatment with TCS alone. However, after stabilization of the condition, in the phase of maintenance therapy, the situation changes: using only moisturizers for four weeks becomes fully equal in effectiveness (SCORAD, POEM, itch intensity) to the results of TCS.
It is the combination of safety, accessibility, and low cost that determines why the working group considers moisturizers as priority means. At the same time, specialists recommend only hypoallergenic formulas and point patients toward the danger of using sensitization-causing additives (for example, plant extracts).
Alongside moisturizers, bathing practices play an important role in the management of atopic dermatitis. Despite the scarcity of evidence, this component is still presented in the guideline in the form of a conditional recommendation.
Studies involving small pediatric groups failed to reveal a significant difference in clinical indicators (EASI, POEM) between the use of soap or bathing frequency (daily vs. twice weekly). Moreover, specific bath additives did not confirm improvement in quality of life and sometimes even caused a slight increase in side effects. However, a 15-20 minute “soak-and-seal” procedure performed twice a day showed a significant decrease in the SCORAD index compared to short bathing. Given these data, the use of hypoallergenic cleansing agents remains advisable.
Along with hygienic procedures, under conditions of professional supervision, a conditional recommendation also applies to diluted bleach baths. A meta-analysis of eight studies confirmed that this method significantly improves clinical indicators (EASI), which is likely explained by a reduction in staphylococcal colonization.
While symptoms assessed by patients (POEM, itch) and quality of life do not essentially change during this time, the safety profile of the method is still evaluated positively. However, to avoid skin irritation, proper dilution of the solution requires special attention.
In searching for additional therapeutic means, inpatient data also provide conditional support for wet wrap therapy. The study showed that the combination of hydrocortisone and 24-hour wet wrapping equals standard care—emollients and topical steroids—in effectiveness (SCORAD). However, since an optimal treatment protocol is not finally established, caregiver burden, unpredictable enhancement of steroid effects, and the preservation of infant safety remain the main challenges.
Prescription Local Pharmacotherapy
Topical corticosteroids (TCS) represent the cornerstone of treatment, with a strong recommendation. This approach is reinforced by their FDA-approved effectiveness and long history of safety. The selection of the preparation’s potency is directly dependent on the anatomical site, severity of the disease, the patient’s age, and the body surface area.
For example, for the face, neck, genitals, and skin fold areas, low-potency means are more acceptable. High or very high-potency agents (e.g., clobetasol 0.05% foam) provide a high probability of complete or almost complete skin clearance (IGA 0/1) in adolescents. Medium-potency options (including mometasone 0.1%) are completely safe even during facial atopic dermatitis in infants.
In patients aged 6 months to 18 years, maintenance therapy with fluticasone 0.05% twice weekly significantly reduces the SCORAD index and the probability of flares. Low or medium-low activity preparations (e.g., hydrocortisone butyrate 0.1%) ensure effective suppression of itching and prevention of recurrences. Although patients have a fear of developing skin atrophy, the correct, intermittent use of these means establishes an optimal balance between rapid symptom management and high safety.
In parallel with topical corticosteroids, topical calcineurin inhibitors (TCIs) deserve a strong recommendation, which is explained by their steroid-sparing profile and the absence of atrophy risk. Tacrolimus ointments facilitate skin clearance in pediatric patients, and when used in the form of proactive therapy, effectively hinder recurrences. Importantly, large-scale studies did not confirm a link between these preparations and oncological pathologies.
Pimecrolimus 1% cream ensures significant improvement in skin condition (IGA 0/1) and long-term prevention of flares. Its use is safe even under 2 years of age, despite the fact that this is formally considered an off-label practice. A local burning sensation may manifest at the initial stage of therapy, although this symptom is short-lived and disappears on its own. It is noteworthy that Health Canada, based on a 2021 review, fully removed the existing warning about malignancy from the preparation’s annotation.
Phosphodiesterase-4 inhibitors also maintain a strong position in modern standards of local therapy. Crisaborole ointment, used from 3 months of age, confirmed high effectiveness in terms of EASI index improvement and flare prevention, although discomfort caused during application sometimes hinders the treatment process. Against this background, roflumilast cream is considered a more convenient alternative for patients, as it practically doubles the probability of achieving EASI75 and, moreover, is characterized by relatively fewer episodes of burning.
In the new stage of therapy, a special place is assigned to ruxolitinib cream (a Janus kinase inhibitor), the use of which is strongly recommended from 2 years of age. The mentioned preparation equals strong corticosteroids in effectiveness and is distinguished by a reliable safety profile during long-term therapy. Nevertheless, an official warning (boxed warning) still limits its area of use to 20% of the body surface.
Another promising means represents tapinarof cream, which is an aryl hydrocarbon receptor agonist and sharply increases the probability of achieving EASI75. It ensures effective itch management and improvement of the IGA index, although slight follicular side effects may still manifest in patients.
Unlike specific therapeutic agents, the use of local antimicrobial means during non-infected atopic dermatitis is not recommended. Systematic reviews confirmed that the inclusion of these preparations in the treatment process does not cause improvement in the SCORAD index, itch intensity, or quality of life. Moreover, their non-targeted use is clinically unjustified because it significantly increases the risks of antibiotic resistance and sensitization.
Phototherapy Options
In case of local therapy ineffectiveness, phototherapy is assigned a conditional recommendation for managing moderate to severe forms of atopic dermatitis. An updated Cochrane review and pediatric studies confirm that the use of narrow-band UVB or UVA1 rays significantly reduces the severity of the disease. However, despite the high therapeutic effect, the mentioned method requires 2-3 sessions per week and, accordingly, a large resource of time.
As for psoralen plus UVA (PUVA) therapy, due to a deficit of pediatric data, the guideline issues a conditional recommendation against its use. This restriction is linked to the high risk of developing skin cancer, specifically squamous cell carcinoma.
Systemic Therapy
Systemic therapy is intended for those complex cases when optimized local means cannot ensure effective control of the disease. The treatment strategy is based on a joint decision with the patient, which requires a complex assessment of disease severity, impact on quality of life, expected effectiveness, safety, and availability of medications. It is noteworthy that this approach is often prescribed in combination with local therapy.
Monoclonal antibodies maintain a leading position and strong recommendation in systemic treatment. Prominent among them is dupilumab (from 6 months of age), which, along with complete skin clearance (IGA 0/1), ensures significant improvement in clinical indices (SCORAD, POEM), itch, and quality of life. The preparation is dosed once every four weeks (main side effect—conjunctivitis).
In adolescents, tralokinumab, lebrikizumab, and nemolizumab also successfully achieve a reduction in EASI and IGA indicators in combination with local therapy. It is noteworthy that nemolizumab is effective even from 6 years of age and is characterized by a low frequency of serious side effects. As for omalizumab, due to insufficient and contradictory evidence in pediatric practice, the guideline does not support its use.
In modern guidelines, oral JAK inhibitors are also assigned a strong recommendation. Above 12 years (and in the case of baricitinib—from 2 years), their use ensures a radical improvement in the clinical picture and rapid symptom management. Although the expected side effects (acne, headache, respiratory infections) are mostly of a mild nature, due to special safety warnings, strict laboratory control of patients remains an essential requirement.
Alongside innovative means, immunosuppressants and antimetabolites also deserve conditional support under conditions of systemic control. For example, the use of cyclosporine is advisable only for a short period, for a maximum term of one year. As for methotrexate, it practically equals cyclosporine in effectiveness, although its advantage lies in prolonging remission and the relatively slow development of recurrence.
In the case of mycophenolate mofetil, a therapeutic response is recorded in 77% of patients. Azathioprine, after preliminary genetic screening, significantly improves disease severity, itch intensity, and quality of life.
The guideline unequivocally distances itself from the long-term use of systemic corticosteroids. This strict position is explained by the high risk of recurrence and such serious complications as damage to the skeletal system or growth retardation in children. Their use is permissible only during acute conditions, in the form of a temporary “bridge” until transitioning to other therapeutic means. As for other systemic agents, due to the absence of solid evidence, recommending them at this stage is impossible.
Cost Considerations and Research Gaps
When selecting a treatment strategy, the financial factor plays one of the decisive roles. Although the effectiveness of biological preparations and JAK inhibitors is reinforced by incontrovertible evidence, their high cost often creates the necessity for insurance coverage.
In parallel, certain research gaps still remain in the scientific literature; specifically, the optimal composition of moisturizers is to be specified, and the exact protocols for wet wrapping and bathing are not finally formed. Direct comparisons of new preparations with already existing, traditional means (TCS/NB-UVB) also require additional study.
Source: JAAD
