
How much does a woman’s reproductive health depend on her social status?
We often view menopause as a genetically predetermined event, but the reality is far more complex: biological processes do not occur in isolation. This stage of life is a reflection of the socioeconomic environment, in which a woman’s education, financial stability, and access to healthcare services play a decisive role.
A new study published in the journal BMJ Global Health, which aggregates data from 716,648 women across 44 countries, has demonstrated the global scale of early-onset menopause. Observations from low- and middle-income countries (LMICs) confirmed that this is not merely a challenge for the healthcare sector; alongside biological factors, this phenomenon is directly linked to social inequalities within society.
What is Early Menopause and Why Does It Warrant Attention?

Menopause—the permanent cessation of menstruation associated with the depletion of ovarian follicles—typically occurs between the ages of 45 and 55. However, when this process begins before age 45, it is referred to as early menopause, and before age 40, it is called premature menopause. Rather than a simple shift in physiological timelines, this is a clinical condition that exerts a serious, long-term impact on a woman’s health.
Women experiencing early menopause face a significantly higher risk of developing cardiovascular diseases. Studies confirm that:
The threat of coronary heart disease is increased by approximately 1.5 times.
The risk of stroke is increased by 1.3 times.
The likelihood of type 2 diabetes is also increased by 1.3 times.
Added to these are elevated probabilities of osteoporosis, cognitive decline, depression, and premature mortality. Beyond these chronic risks, early menopause causes daily discomfort: hot flashes, urogenital changes, and psychological distress significantly disrupt a woman’s quality of life. Unfortunately, in many low- and middle-income countries, these women have limited access to diagnosis and treatment, which further exacerbates their condition.
The Global Scale of the Problem
The new paper published in the journal BMJ Global Health utilizes the extensive database of the Demographic and Health Surveys (DHS). This standardized survey, covering more than 90 low- and middle-income countries, is a vital informational resource for assessing women’s health status.
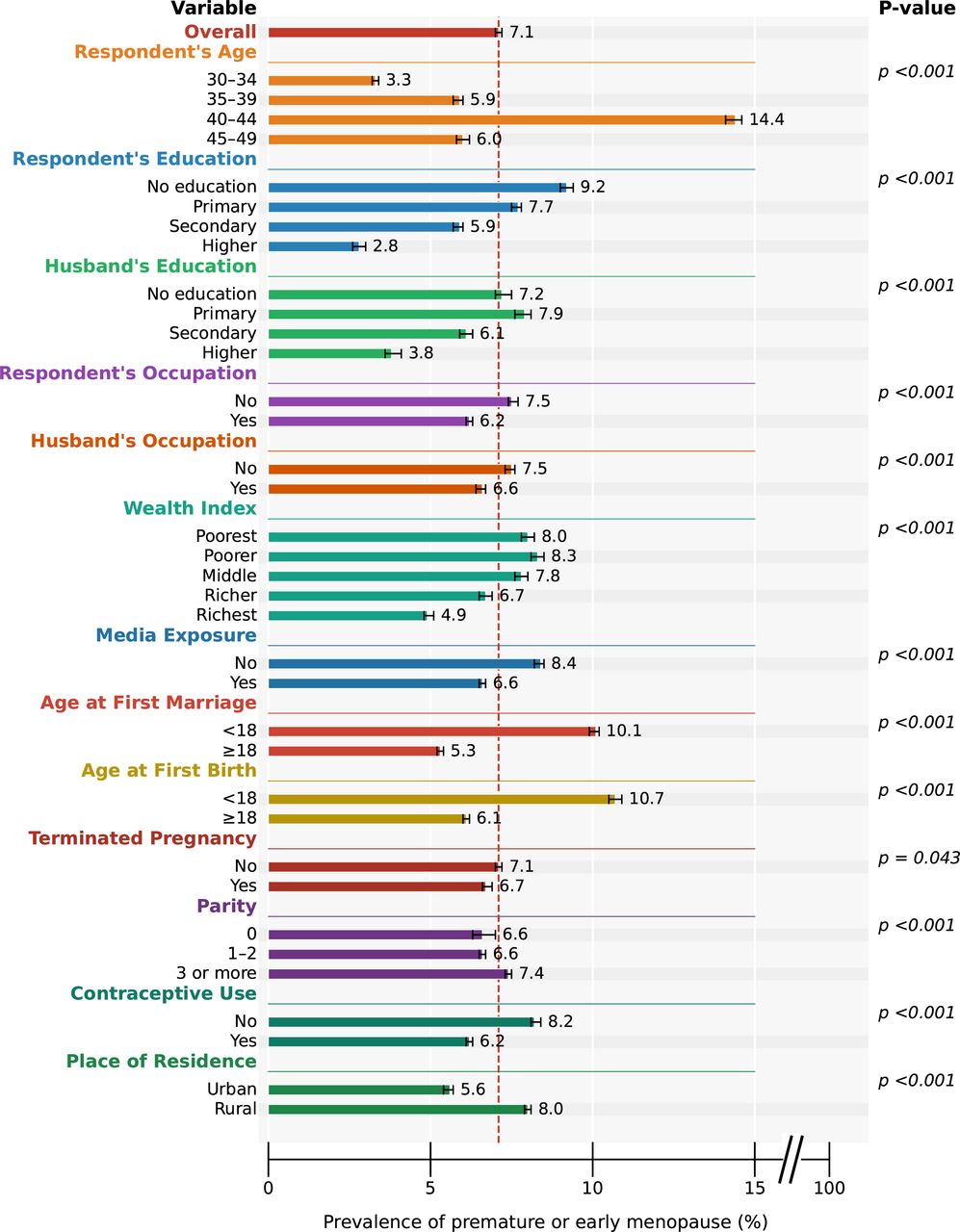
The study’s findings reveal that the prevalence of early and premature menopause in the studied countries reaches 7.1%, meaning that this condition affects approximately one in fourteen women. This figure is significantly higher than previous global estimates, which relied primarily on data from high-income countries and estimated the prevalence of premature ovarian insufficiency at just 3.5–3.7%. The new data also fully align with evidence documenting a heavy burden in developing nations, matching trends observed in Sub-Saharan Africa and regions of Asia.
Scale is of decisive importance here. Against the backdrop of rapid population aging in low- and middle-income countries—where an increasing portion of women’s lives is spent in the postmenopausal period—this level of prevalence imposes a heavy burden on healthcare systems that already operate with limited resources and face numerous challenges.
Variations Across Countries
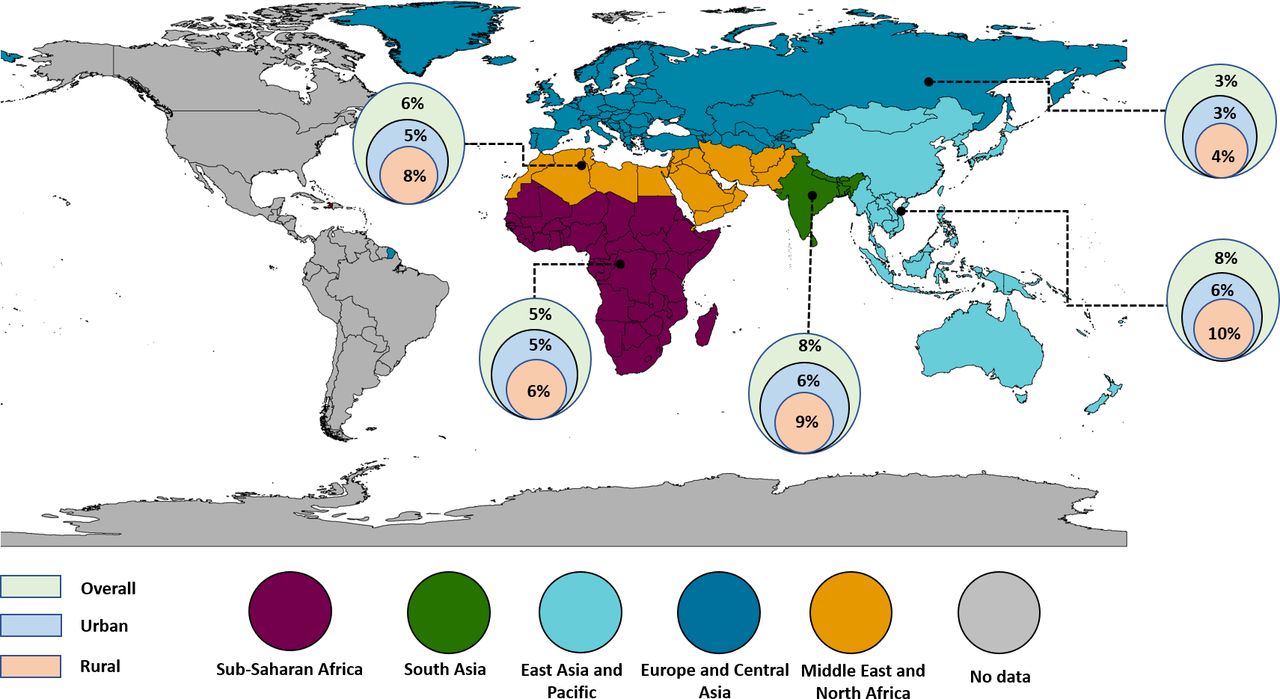
One of the critical findings of the study is regional heterogeneity: the prevalence of early and premature menopause varies significantly between countries, ranging from 2.3% in Jordan to 12.0% in Ethiopia. The highest rates were recorded in Ethiopia, Indonesia, and Myanmar, while the lowest were found in Jordan, Gabon, and Armenia.
This disparity indicates that a country’s general economic status or geographic location alone is not the deciding factor. The real impact is driven by local determinants: early marriage, nutritional quality, healthcare access, and environmental exposures.
Ethiopia’s high rates are fully consistent with concomitant issues of malnutrition, early marriage, restricted healthcare access, and indoor air pollution.
Conversely, the countries with the lowest prevalence are characterized by high levels of urbanization, better education, and developed healthcare infrastructure. For example, in Middle Eastern and North African countries, where the practice of early marriage is less common and female education receives more emphasis, the rates are significantly lower.
By region, the rate of early menopause is 7% in Western Pacific countries, 12% in Southern Africa, and rises to nearly 15% in South and Southeast Asia. These statistics highlight significant challenges in some of the world’s most densely populated regions.
Urban vs. Rural: Regional Disparities
An equally important finding of the study is the stark contrast between urban and rural areas. According to the data, the prevalence of early or premature menopause among rural women stands at approximately 8%, exceeding the rate in urban areas. Even after adjusting for other socioeconomic factors, rural women are 17% more likely to develop this condition than their urban counterparts.
This difference is easily understood when examining the underlying causes. Rural women in low- and middle-income countries face a much higher risk of early marriage and early childbirth, both of which were confirmed as independent risk factors in this study. They are also more heavily exposed to strenuous physical labor, agrochemicals, and occupational hazards.
Furthermore, due to limited access to primary healthcare services, detecting and treating reproductive health issues at an early stage is highly complicated. Nutritional deficiencies are also widespread, and low awareness about menopause prevents women from seeking timely assistance, leaving the true scale of the problem obscured.
The Role of Education: Protecting Reproductive Health
The study revealed an inverse relationship between education level and the risk of early menopause. The results are clear: women with no formal education show the highest rate of early menopause at 9.2%. As the level of education rises—from primary to secondary or higher—the likelihood of developing this condition decreases proportionally.
These findings align with global trends. A systematic review conducted across 24 countries demonstrated that women with higher education enter menopause an average of seven months later than those with lower levels of education. While this is a minor difference on an individual level, across a population it translates into a substantial reduction in risk. For example, a study conducted in India demonstrated the critical impact of educational disparities, recording a sevenfold difference in the prevalence of premature menopause between the most and least educated women.
The reasons behind this phenomenon are complex. Women with higher education typically exhibit better nutritional status, reduced chronic stress, and high health literacy. Reproductive behaviors characteristic of this group—including a later age at childbirth—act as protective mechanisms.
Additionally, better access to healthcare services and fewer unnecessary gynecological interventions contribute to this outcome. Specifically, this includes the limitation of hysterectomies—which act as a cause of iatrogenic menopause—and the use of more conservative approaches for benign conditions, which in turn is a crucial prerequisite for preserving a woman’s reproductive health. These findings confirm once again that investing in girls’ secondary education is not merely a matter of gender equality; it is one of the most effective strategies for improving women’s health.
Early Marriage and Childbirth: The Heavy Burden of Inequality
Early marriage and early childbirth have a direct and severe impact on a woman’s reproductive health. The data are clear:
Among women married before age 18, the prevalence of early or premature menopause is 10.1%, whereas for those married at age 18 or older, this figure is only 6.5%.
A similar trend is documented in childbirth, where the rate reaches 10.7% among women who first gave birth before age 18.
The study demonstrated that women who married or first gave birth after age 18 have a 34% and 25% lower risk, respectively, of developing early menopause.
What mechanisms underlie these outcomes? From a biological perspective, adolescent pregnancy imposes a significant metabolic demand on the body, as maternal physical development is still ongoing, and the partition of micronutrients between mother and fetus becomes highly competitive. This process is accompanied by a higher risk of sexually transmitted infections, which predisposes to the development of pelvic inflammatory disease and subsequent ovarian dysfunction. Furthermore, the elevated frequency of obstetric complications during adolescent pregnancies increases the necessity for surgical interventions, which, in turn, leads to the depletion of the ovarian follicular reserve.
However, a biological explanation alone is insufficient. Early marriage and childbearing are indicators of socioeconomic disproportion, closely linked to poverty, educational deficits, and restricted access to healthcare. These factors reflect the influence of patriarchal structures and the restriction of girls’ autonomy, which prompts families to marry off their daughters prematurely due to economic pressures. Consequently, early menopause transcends a narrow medical context, serving as a long-term reflection of social inequalities that restrict girls’ developmental potential at the earliest stages of life.
Multiparity as Biological Protection
One of the most intriguing findings of the study is that high parity—specifically, having three or more children—significantly reduces the risk of early menopause.
At first glance, this might seem counterintuitive. Given the major physiological shifts within a woman’s body, it is often assumed that pregnancy exhausts the organism and depletes reproductive resources rapidly. However, the reality is different: menopause occurs when the ovarian follicular reserve is depleted. Each pregnancy halts ovulation for approximately 9 to 12 months, and breastfeeding—depending on its intensity—extends this period by another 6 to 24 months. During this time, the ovaries “rest,” follicles are not expended, and the body effectively preserves its reserve.
Consequently, women who have experienced multiple pregnancies undergo fewer total ovulatory cycles over their lifetimes, depleting their follicular reserve more slowly and reaching the threshold of menopause later. The opposite is observed in women who have never had children (nulliparous women): they lack these “anovulatory breaks,” which often leads to menopause occurring at an earlier age. This mechanism of ovulatory suppression is biologically fully justified and has been confirmed by numerous large-scale studies.
Socioeconomic Factors
The relationship between higher household economic status and early menopause proved to be more multifaceted than initially appeared. Based on superficial analysis, women in financially stable households had a lower probability of developing this condition. However, once education, place of residence, and other factors were controlled for, the picture shifted: in reality, the highest risk of early menopause was observed precisely among women of middle-income status.
Why is this the case? The authors hypothesize that this is explained by the nutritional transition occurring in low- and middle-income countries. Within the middle-income cohort, lifestyle changes are frequently accompanied by an increase in body mass index (BMI) and elevated metabolic risks.
The issue is further compounded by uneven approaches in the healthcare system: despite increased access to surgical interventions, the quality of conservative management for gynecological pathologies is often low. Consequently, even for benign conditions, hysterectomies are frequently performed, ultimately precipitating artificial, iatrogenic menopause in patients.
Regarding employment, the picture is different: employed women exhibit a lower likelihood of early menopause. This finding can be explained by material advantages (good nutrition, financial security) as well as social integration and psychosocial well-being.
However, it is essential to consider the possibility of “reverse causality”: it is entirely possible that early menopausal symptoms prompt women to leave the labor market, creating the false impression that employment itself reduces the risk. Furthermore, the working conditions themselves are of critical importance—strenuous physical labor, contact with harmful chemicals, shift work, and chronic stress exert a negative influence on the reproductive system and accelerate the aging process.
Beyond the Numbers: An Invisible Healthcare Crisis
The most alarming conclusion of the study is not the statistical data, but the neglect of the context in which these women live. Although menopause is a natural and inevitable phase of a woman’s biological cycle, in the majority of low- and middle-income countries, it is entirely omitted from political and healthcare agendas.
The current reality is stark: clinical guidelines are extremely limited, medical personnel lack the appropriate qualifications or training in menopause management, and screening protocols are virtually nonexistent. The majority of women do not receive evidence-based treatment, including hormone replacement therapy, which is essential for many. Most disturbingly, these services are least accessible to those who need them most—rural, less-educated women living in countries where the scale of this problem is highest.
Limitations and Strengths of the Study
The authors critically analyze the study’s methodological limitations:
The cross-sectional design does not allow for the precise establishment of causal relationships. While the identified associations are consistent with the proposed mechanisms, the risk of residual confounding factors remains.
Notable among the limitations is the subjectivity of the data, which relies on the accuracy of self-reported information from respondents.
Furthermore, the use of a 6-month threshold to identify menopause (instead of the WHO-recommended 12 months) might reduce classification accuracy; however, it is worth noting that sensitivity analyses verified with a stricter methodology yielded nearly identical results.
In the analytical portion of the study, precisely differentiating users of injectable hormonal contraceptives from women experiencing natural or surgical menopause presented a challenge.
Additionally, the lack of important variables within the Demographic and Health Surveys database—such as smoking, physical activity, diet, and environmental factors—somewhat hinders a deeper interpretation of the study’s findings.
Despite these methodological limitations, the study is outstanding in its scale: a standardized analysis of data from 716,648 women across 44 countries provides an evidence base that cannot be achieved within localized studies. The accuracy of the findings, their biological validity, and their consistency with earlier research reinforce the argument that these results should serve as a foundation for future systemic reforms.
Source: BMJ Global Health
