Historically, the process of eating has been associated for many people with chronic distress, manifested by pain localized in the epigastric area, a feeling of post-prandial heaviness, or nausea. Even in the era of Hippocrates, this symptom complex was referred to by the name of “dyspepsia,” which generally denoted a disturbance of the digestive system’s function. However, before the introduction of modern diagnostic methods, it was difficult to draw a line between evident structural damages (such as a peptic ulcer) and functional disturbances that do not possess a visible organic basis.
At the beginning of the 20th century, doctors from medical institutions such as the Mayo Clinic focused attention on a category of patients who had a pronounced picture of gastroenterological complaints, although the radiological or visual studies of that time could not record physical damages. Precisely this clinical observation laid the foundation for the term “functional dyspepsia,” which Walter Alvarez established in medical practice in 1916.
According to modern epidemiological data, this disorder affects approximately 7.2% of the world’s population. Statistical analysis shows a gender asymmetry: the condition is recorded 1.6 times more often in women, while the highest rate of manifestation of the pathology is revealed in the age category under 40 years.
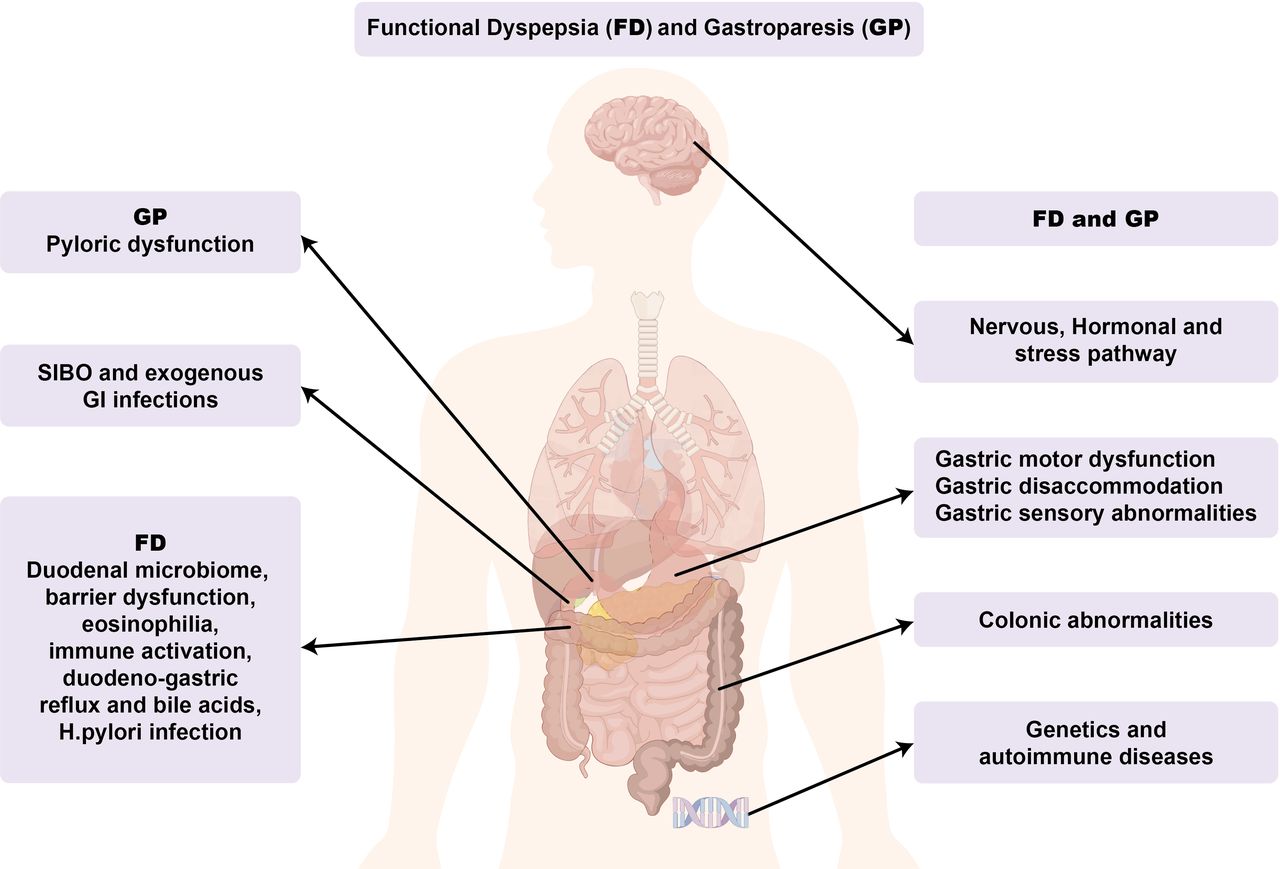
Modern research confirms that complex factors participate in the formation of functional dyspepsia, beginning from changes in the immune response and ending with the disturbance of the microbiota and neuromuscular dysfunction. These mechanisms often create a favorable ground for the manifestation of conditions such as gastroparesis as well. Such a biological intersection makes it clear that functional dyspepsia and gastroparesis are not two independent diseases, but rather different manifestations of a unified clinical spectrum.
Functional Dyspepsia
Functional dyspepsia (FD) is a chronic discomfort syndrome localized in the epigastric area, which proceeds without structural pathology. The clinical symptom complex includes pain, burning, post-prandial (after eating) fullness, and early satiety, which are often accompanied by nausea and meteorism.
Acute gastroenteritis (post-infectious FD forms in 10% of cases) and active tobacco use play a leading role in the etiology of the disease. It is noteworthy that the share of genetic predisposition is minimal and amounts to only 5%, which emphasizes the dominant influence of environmental factors.
In one-third of patients, concomitant psycho-emotional distress (in the form of anxiety or depressive disorders) is recorded. It is noteworthy that the mentioned connection carries a bilateral character: the mental background may represent a predisposition for the disease, although the chronic symptomatology itself often becomes the cause of the worsening of the mental state.
The social burden of the disease and its influence on the quality of life are analogous to other severe chronic pathologies. In 2/3 of cases, the persistence of the condition determines the excessive spending of healthcare resources. In addition, epidemiological data indicate increased risks of hospitalization and mortality, which emphasizes the clinical severity of the nosology.
The clinical picture is complicated by high comorbidity: 33-50% of patients exhibit irritable bowel syndrome (IBS), while 30% have reflux disease (GERD). Such clinical overlap increases the intensity of symptoms and resistance to therapy.
Pathophysiology
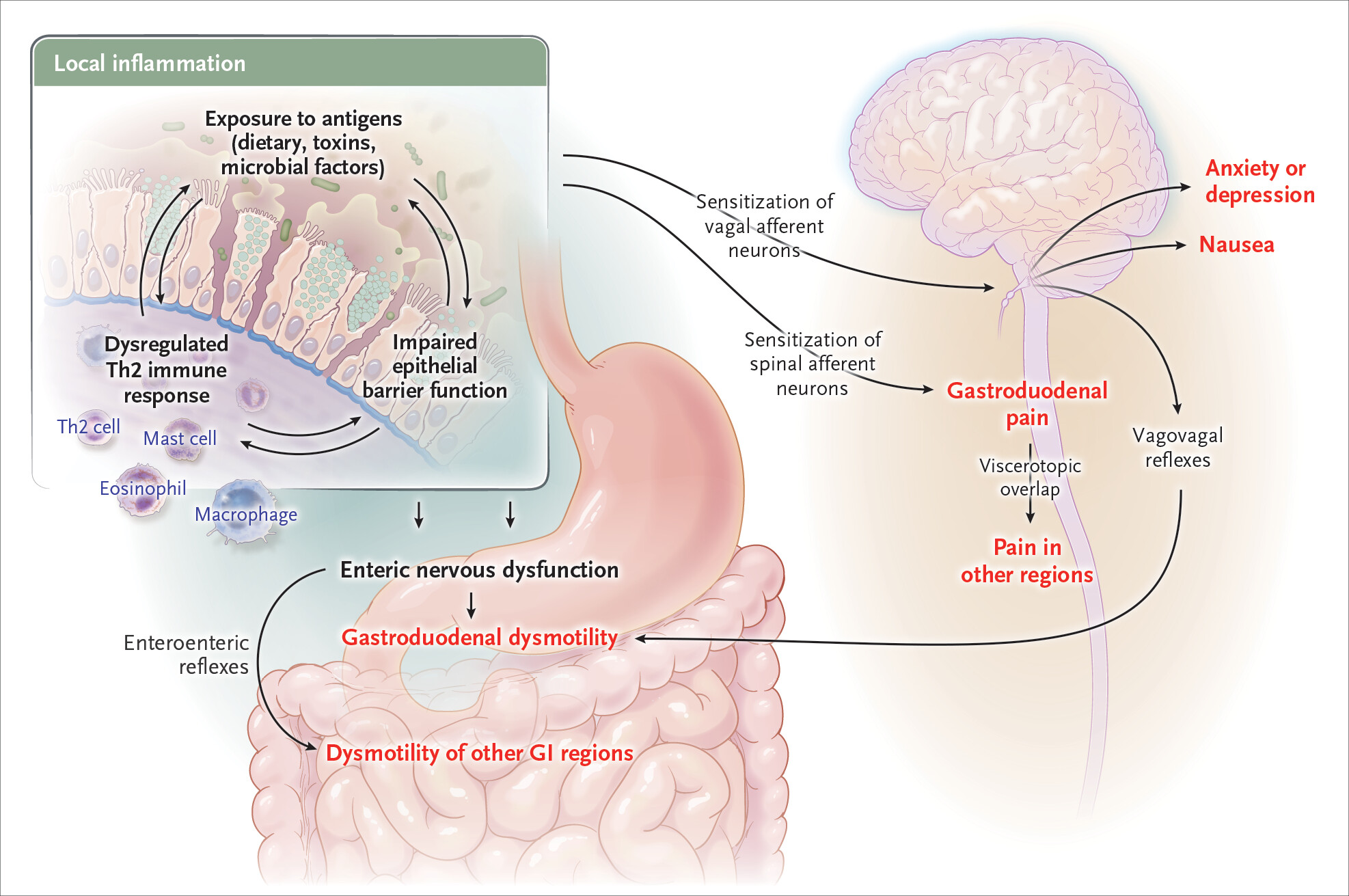
The heterogeneity of functional dyspepsia points to the coexistence of various biological mechanisms. Local micro-inflammation of the duodenum represents a leading link, which is determined by the aberrant immune response of Th2 cells. The severity of clinical symptomatology directly correlates not only with the number of eosinophils and mast cells but also with their activation and degranulation.
The mentioned immune shifts cause neuronal dysfunction and the loss of interstitial cells of Cajal (ICC—the pacemakers of the gastric rhythm), which determines the following motor disturbances of the stomach:
Disturbance of accommodation (revealed in 40% of cases);
Visceral hypersensitivity toward stretching (recorded in 40%);
Delay in gastric emptying (recorded in 30%).
The entry of acidity secreted by the stomach into the duodenum causes the irritation of nerve endings, which hinders the natural relaxation and adaptation of the stomach after the intake of food. General disturbances of the immune system are often connected with allergic manifestations (atopy), diseases of the joints, and their hypermobility. The existence of specific autoimmune signs in a quarter of patients indicates that the problem is not limited only to the stomach and encompasses the entire organism.
Foodborne pathogens, dysbiosis, and environmental allergens are considered as initiators of the pathological process, which is facilitated by the increased permeability of the mucous membrane. Additional factors represent the dysregulation of bile salts and dietary components (salicylates, histamines).
Gastroparesis
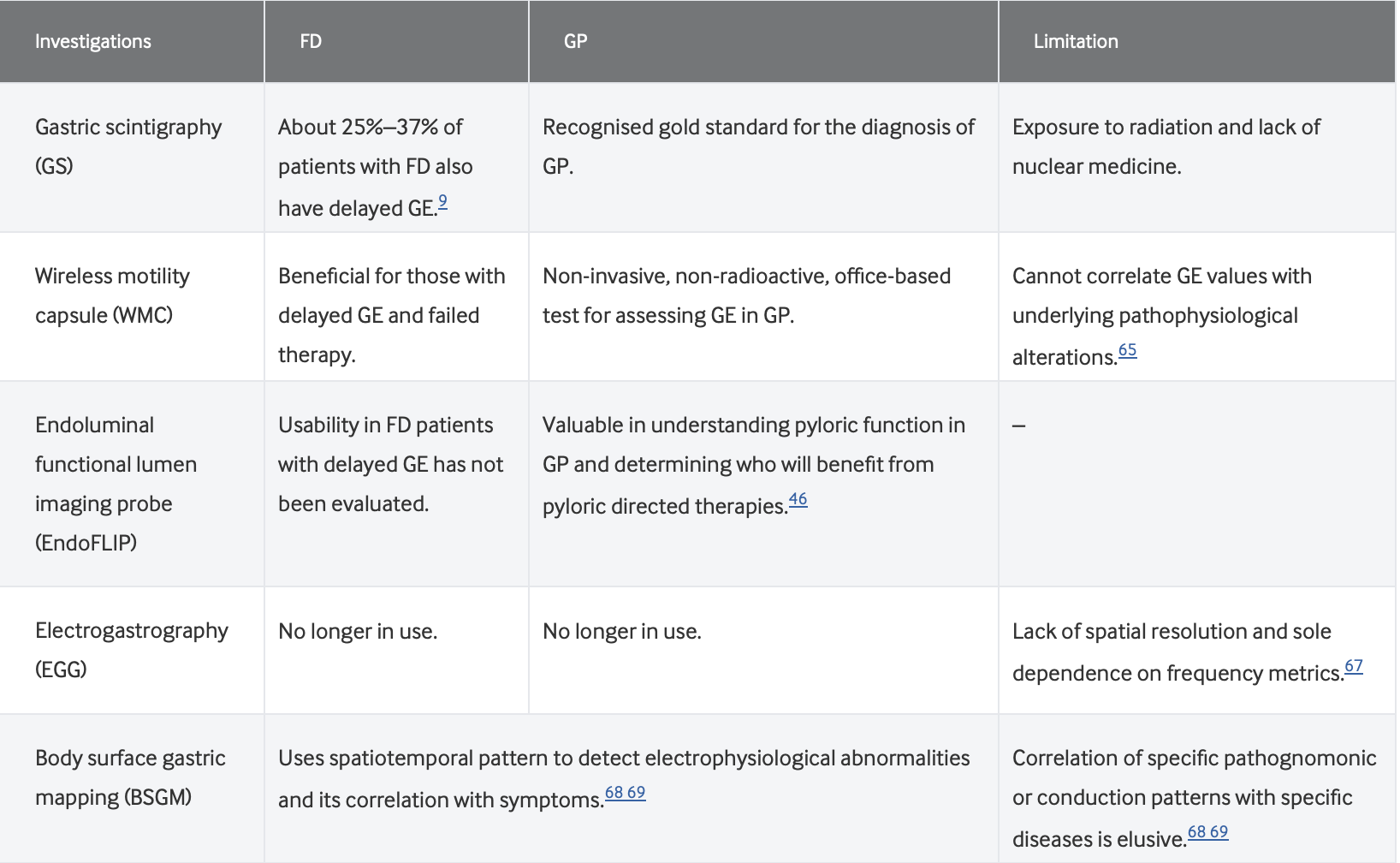
Gastroparesis is a severe neuromuscular disorder that manifests primarily in an idiopathic form. The diagnosis is based on the confirmation of the delay of stomach contents by scintigraphy (>60% after 2 hours or >10% after 4 hours, in the absence of mechanical obstruction). In the clinical picture, nausea (96%) and vomiting (88%) represent the leading symptoms, which are accompanied by post-prandial fullness, bloating, and early satiety.
The pathology manifests much more often in women compared to men. Diagnostic instability is noteworthy, which erases the line between gastroparesis and functional dyspepsia:
In 42% of those diseased with gastroparesis, the stomach’s work normalizes over time;
In 37% of functional dyspepsia cases, the process of stomach emptying is delayed later.
Since the symptoms, clinical severity, and prognosis of both conditions are identical, modern medicine considers them not as separate diseases, but rather as parts of a unified pathological spectrum.
Common Etiopathogenesis: From Infection to Immune Dysfunction
Infectious agents play a decisive role in the development of both conditions. Helicobacter pylori, as well as Salmonella, Giardia, or SARS-CoV-2, trigger a cascade of pathological processes. The infectious process disrupts the natural barrier of the duodenum, which increases the permeability of the mucous membrane. This opens the way for bacteria and antigens, which ultimately causes a microbiome imbalance (dysbiosis). For example, in almost half of those diseased with gastroparesis, small intestinal bacterial overgrowth syndrome (SIBO) is revealed.
The organism responds to the disturbance of the barrier function with specific immune activation. During functional dyspepsia, the accumulation of eosinophils and mast cells (inflammation determined by Th2/Th17) irritates nerve endings, which determines pain and early satiety. In the case of gastroparesis, the immune response carries a more aggressive character and hinders the mechanism of stomach emptying through specific cytokines (CXCL1, IL18) and macrophages.
Nervous and muscular structures represent the main target of this immune attack. The loss of interstitial cells of Cajal is characteristic of both pathologies. Precisely this structural damage disrupts the electrical rhythm of the stomach, which explains the disturbance of accommodation and visceral hypersensitivity. In this way, infection, the microbiome, and immunity create a unified chain that turns a functional disturbance into a chronic pathology.
Diagnostic Strategy
The initial stage of diagnostics implies the exclusion of other pathologies, for which special attention is paid to “alarm signs.” Among these symptoms are named: weight loss, pain that is not connected with food intake, age over 60 years, oncological history, difficulty swallowing (dysphagia), anemia, or bloody vomiting (hematemesis).
The standard protocol envisions universal testing for H. pylori, because the destruction of the bacteria determines remission in 10% of patients. Endoscopic research mostly reveals erosions and ulcers, while it records malignant processes in only 0.4% of cases.
In those patients who exhibit nausea and vomiting, diagnostic priority is given to scintigraphy. An innovative method, body surface gastric mapping (BSGM), helps us in identifying disturbances of the organ’s electrical rhythm, which is in direct connection with the severity of symptoms.
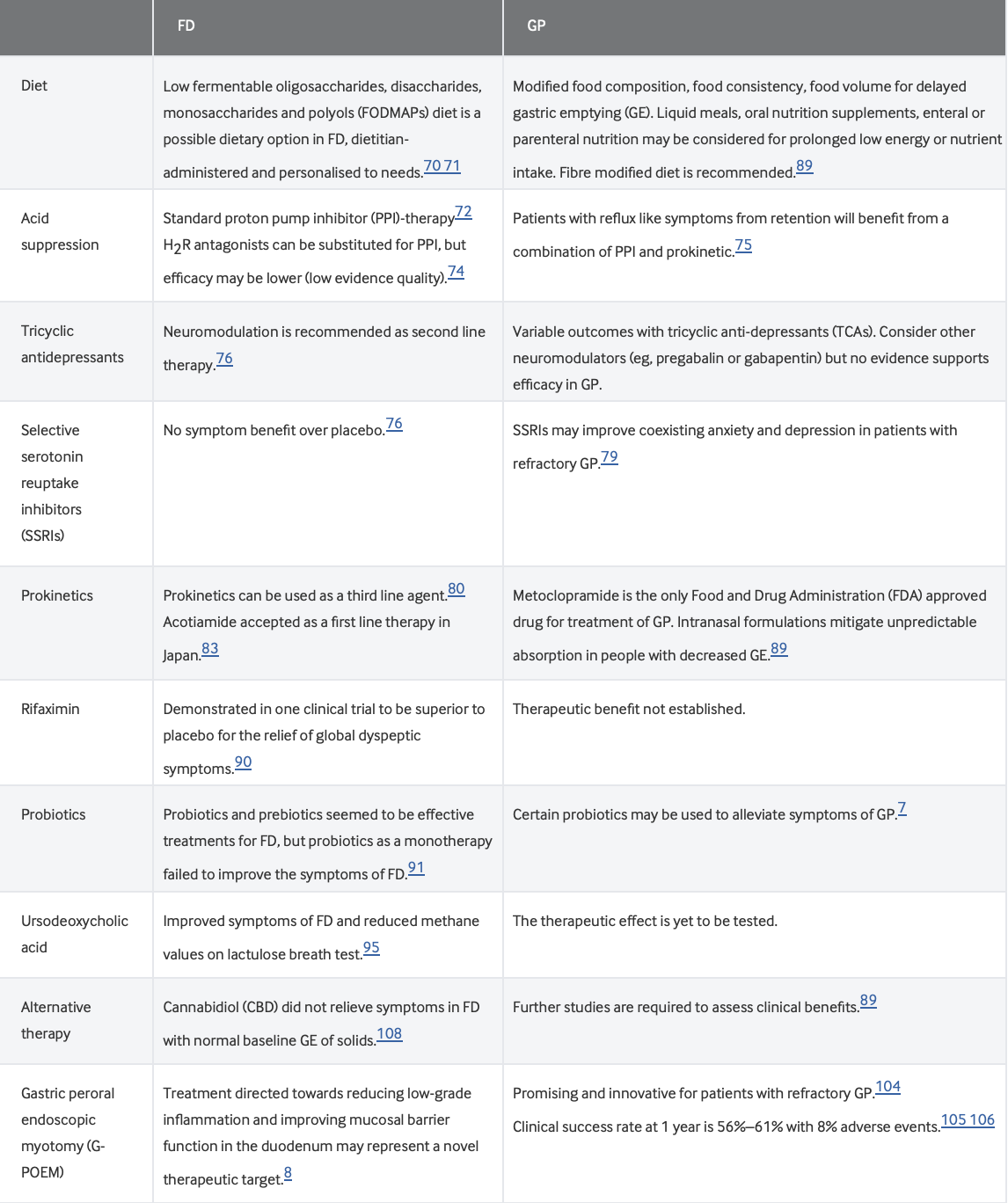
Complex Management
Since officially approved medications for functional dyspepsia do not exist, the treatment carries a symptomatic character and first of all relies on an individually selected diet. This approach implies frequent eating in small portions and the restriction of fatty, carbonated, or spicy products.
The therapeutic arsenal envisions the suppression of the acidic environment with proton pump inhibitors (PPIs), which reduce eosinophilic inflammation along with symptoms.