
The primary barrier in treating Type 1 diabetes is the local suppression of autoimmune aggression. Managing the focus of inflammation while bypassing systemic immunosuppression has proven to be such a complex task that it remained an unresolved problem for decades.
The situation is further complicated by the polyclonal nature of the immune response. This means that insulin-producing beta cells are simultaneously targeted by various types of “aggressor” lymphocytes. Under conditions where existing therapeutic approaches cannot provide full control over a multifaceted immune assault, bispecific molecules offer an alternative path for forming immunotolerance.
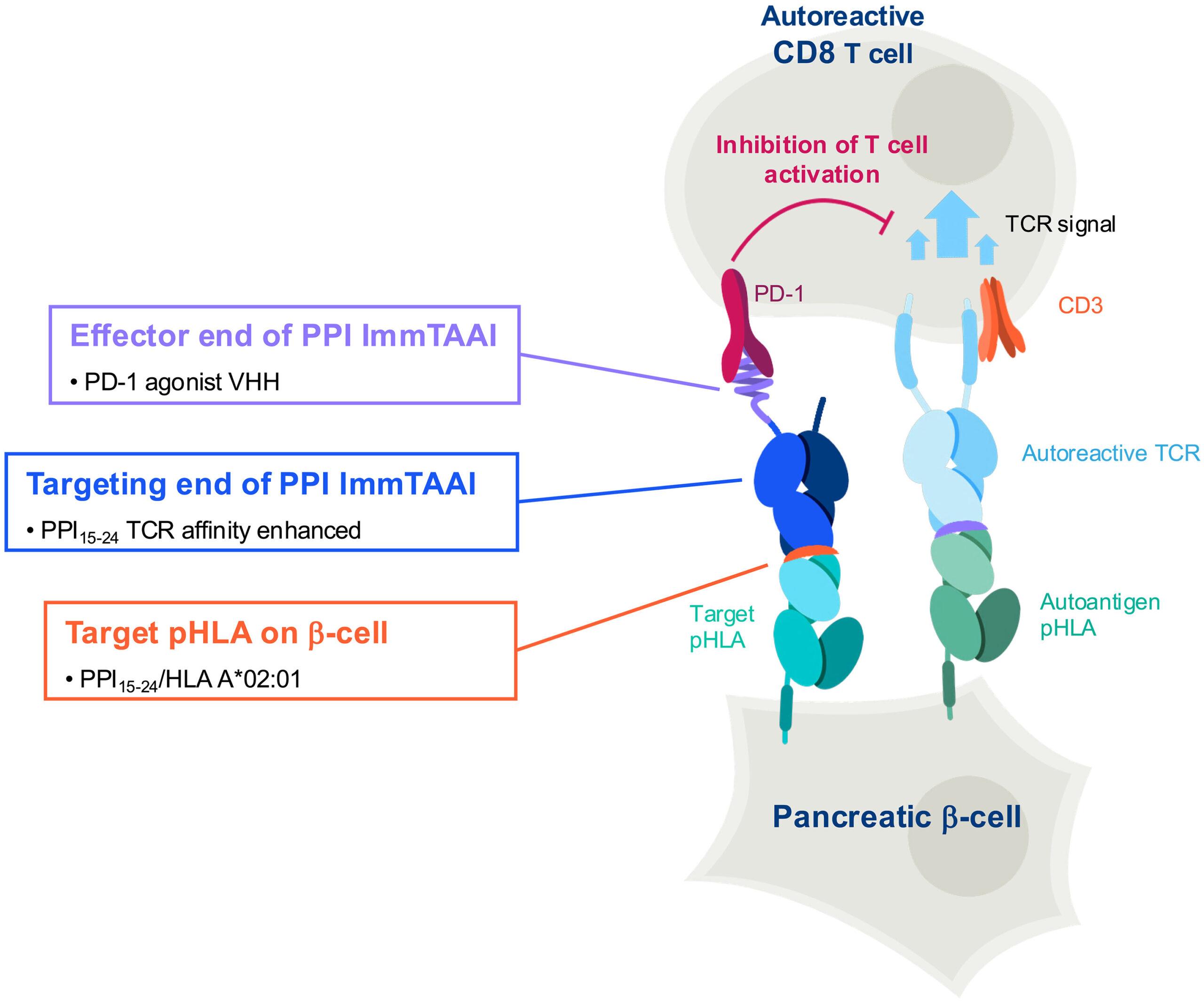
The foundation of this innovative approach is ImmTAAI, which embodies a bifunctional “bridge” by its nature. Its targeting domain selectively binds only to beta cells, while the effector part sends a “calming” signal to aggressive T-cells (via the PD-1 receptor). This dual action ensures a localized and targeted cessation of the immune attack.
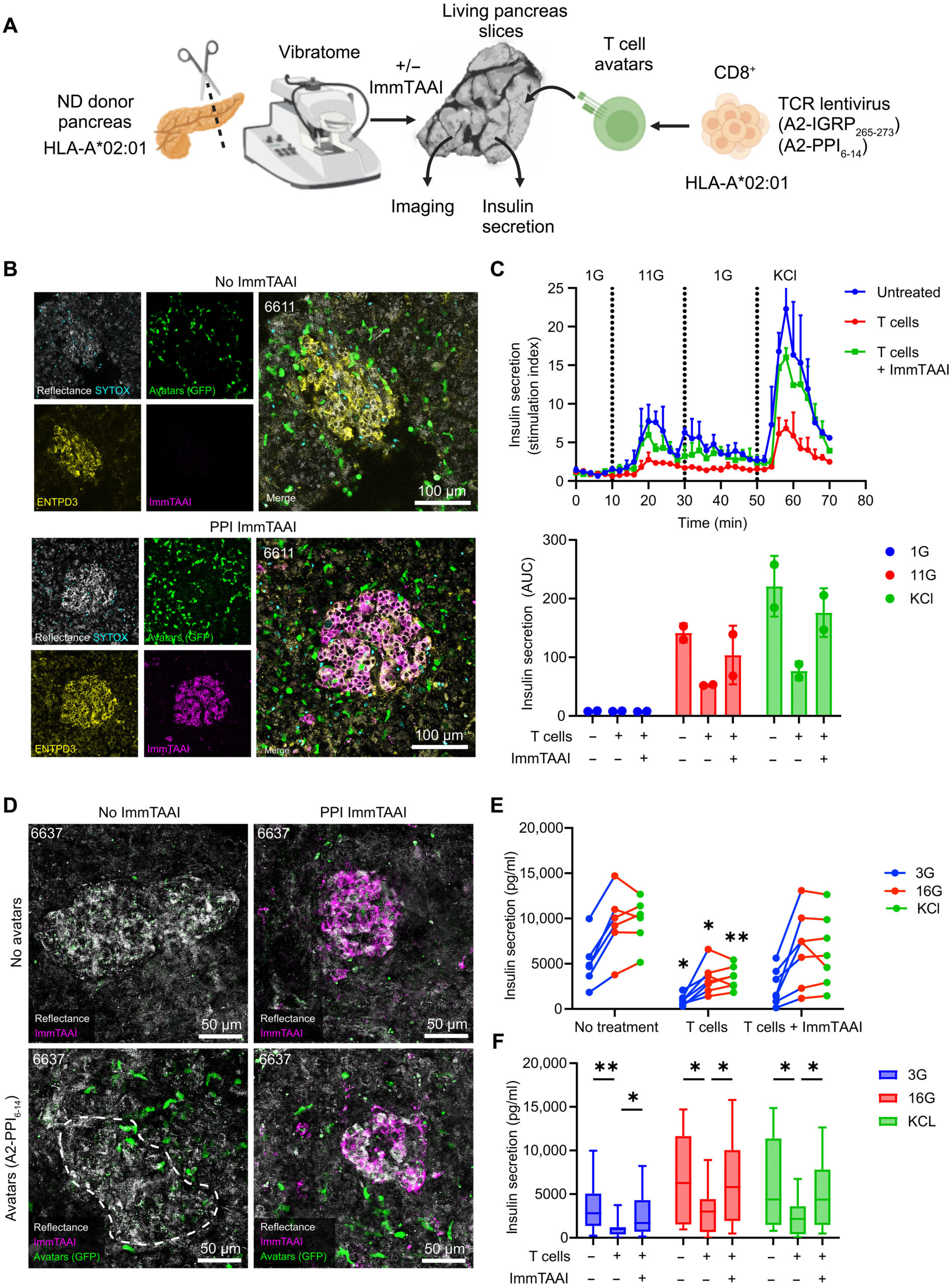
The “conditional activation” design of ImmTAAI results in high therapeutic safety. It activates only after binding with the target peptide complex; until then, it maintains a completely inert state in the bloodstream. To validate this mechanism, researchers used native fragments of pancreatic tissue 120 μm thick. This model increases the validity of the research by preserving tissue physiology.
The Role of the PD-1/PD-L1 Pathway in Maintaining Immune Tolerance
The PD-1/PD-L1 pathway plays a decisive role in the pathogenesis of Type 1 diabetes as a central link in immune self-control. The system serves to restrain pathogenic lymphocytes and neutralize their destructive potential. Notably, the expression of PD-1 in pancreatic infiltrate represents a constant biological reality. This phenomenon is recorded with identical precision in both experimental models and human tissues. Consequently, any disruption of this protective barrier—including genetic—significantly accelerates the progression of diabetes.
Clinical studies conducted for treating the disease assign particular importance to the protective function of PD-1. Practical data confirm that an effective therapeutic response is often established precisely on the activation of this receptor. However, the full execution of the process requires the synchronous involvement of the T-cell receptor (TCR) and peptide-HLA complexes. It is precisely this peculiarity of tissue-specific pHLA presentation that determines the selective “calming” of the immune system only at the site of damage.
Target-Specific Binding
The research process consisted of three decisive phases, which demonstrated the mechanism of action of ImmTAAI in detail:
Affinity Study: In the first stage, scientists studied the structural stability of ImmTAAI and its attraction force (affinity) to the target. Fluorescent analysis confirmed that the molecule binds to the specific beta-cell complex (PPI15-24:HLA-A∗02:01) with unprecedented precision. In parallel, TCR tests revealed that the drug not only finds the target but also stably induces the necessary immune response.
Tissue Localization: The subsequent step tested the behavior of the molecule in native pancreatic tissue. The experiment revealed the strict selectivity of ImmTAAI: the drug localized only within the islet apparatus and did not establish any contact with other structures. The absolute nature of this specificity was confirmed by a control conducted on HLA-A31 type tissue, where no fixation of the molecule was recorded.
Pathological Simulation: The culmination of the research represented a simulation of the pathological process. For this purpose, researchers used Interferon-gamma, which brings the experiment as close as possible to the clinical picture. It turned out that in a pathological environment, the degree of target cell recognition and fixation by ImmTAAI increases significantly. Accordingly, the inflammation factor represents a kind of catalyst for the molecule’s targeted action.
Prevention of Pathological Immune Contact and Protection of Target Cells
Under the influence of PD-1 agonism, the behavior and movement trajectory of cytotoxic T-cells change qualitatively. In physiological conditions, aggressive lymphocytes establish long-term, stable contact with target cells, which determines their subsequent destruction. However, the use of PPI-ImmTAAI effectively hinders this destructive connection.
Observations conducted in beta-cell co-cultures showed that, under the influence of the drug, the movement speed of specific T-cells increases significantly. This means that the immune agents lose their orientation on the target and can no longer manage to maintain solid contact with them. This effect became particularly visible in islets with inflammatory infiltration, where treatment with ImmTAAI returned the lymphocytes’ movement capability to within normal limits.
Ultimately, the molecule successfully disrupted the harmful interaction between beta cells and lymphocytes. The therapeutic effect is achieved not by the direct destruction of immune cells, but by modifying their behavior, which ensures the neutralization of aggression at the site of damage.
Suppression of Cytotoxic Function
To model the autoimmune process with maximum precision, researchers used so-called “avatars” of CD8+ T-cells. These cells express islet-specific receptors (TCR), which allowed them to successfully achieve targeted breakdown (lysis) of beta cells. However, the involvement of PPI-ImmTAAI in the process radically changed the situation.
The molecule sharply suppressed cytotoxic activity under all studied ratios. This protective effect was analyzed in depth by studying the multiplex cytokine profile. The research also showed a coordinated decline in effector molecules—granzymes, perforin, and TNF.
In the end, ImmTAAI creates a two-sided barrier: it not only physically distances the lymphocyte from its target but also effectively neutralizes its biochemical arsenal. Under the influence of the drug, aggressive cells completely stop secreting the toxic substances necessary to damage beta cells.
Clinical Translation Potential and Limitations
The possibility of the practical realization of ImmTAAI is made even more real by its design. The structure of the drug repeats the model of an already approved medication—tebentafusp. The latter represents the first bispecific TCR therapy authorized by the FDA, which significantly increased patient survival rates in oncology. Consequently, using such a technological platform determines the clinical validity and safety of the new drug.
The transfer of the technology for treating Type 1 diabetes (T1D) is also simplified by the genetic profile of patients. The high prevalence of the HLA-A∗02:01 allele in persons diseased with T1D fully supports the rapid clinical evaluation of this new therapy. This circumstance allows for a large target population and the possibility of operatively implementing the next phases of the research.
Ultimately, a successful therapeutic precedent and favorable genetic prerequisites create a solid foundation for implementing ImmTAAI into clinical practice.
However, alongside methodological advantages, the work includes certain objective limitations. The main challenge in the research process was the shortage of human pancreatic tissue and the short period of its cultivation in laboratory conditions. This time frame somewhat complicates the long-term modeling of the chronic progression of Type 1 diabetes. Accordingly, it is necessary to take this factor into account when planning further research.
Source: Science Advances
