
Sepsis represents a life-threatening, dysregulated response of the organism to infection, which is characterized by such severe pathological processes as systemic inflammation, immunosuppression, vascular damage, and organ dysfunction. On a global scale, this condition is responsible for 48.9 million cases and 11 million fatal outcomes annually. During septic shock, mortality approaches 40%, which makes sepsis one of the primary causes of repeated hospitalization and healthcare economic costs.
Taking these challenges into account, the 2025 Emergency Medicine Practice review is focused on those critical contradictions that exist between regulatory norms (CMS SEP-1), international guidelines (Surviving Sepsis Campaign 2021), and the latest clinical data. On the basis of a systematic analysis of 1,052 latest publications, the present work establishes effective strategies for the early recognition of sepsis and resuscitation measures.
Pathophysiological Mechanisms
The process of sepsis development begins when the organism loses control over a local infection and the immune response takes on a chaotic, systemic character. In the initial phase, there is a massive expression of pro-inflammatory cytokines (TNF-α, IL-1, IL-6), which creates a pathophysiological picture characteristic of a “cytokine storm.” This aggressive environment damages the inner layer of the blood vessels, which for its part causes the formation of microthrombi and an increase in the permeability of capillary walls.
Along with the progression of the pathological process, the compensatory resources of the organism are exhausted and the condition moves into an immunosuppressive phase. At this time, the death of lymphocytes and the exhaustion of immune cells determine the high vulnerability of the organism toward secondary infections. While the long-term disturbance of blood circulation deprives the cells of vital energy, which ultimately ends with the development of multi-organ failure.
The extreme point of this degradation is septic shock, where circulatory and metabolic collapse sharply reduces the patient’s chances of survival. It is also important that only in half of the cases is it possible to confirm the causative agent (bacteremia) directly in the blood. This proves once again that during sepsis the main threat is not the microbe itself, but the uncontrolled reaction of the organism directed at self-destruction.
The Evolutionary Path of the Definition of Sepsis
The early definitions of sepsis (1991 and 2001) were based on the concept of systemic inflammatory response syndrome (SIRS). By these criteria, for the confirmation of the diagnosis, the existence of at least two of the clinical-laboratory signs given below was necessary:
Temperature >38°C or <36°C;
Heart rate >90 beats/minute;
Respiratory rate >20/minute (or <32 mm Hg);
Leukocyte count >12,000/μL, <4,000/μL, or >10% band forms.
In that period, “severe sepsis” implied a condition associated with organic dysfunction, while “septic shock” was defined by hypotension resistant to infusion. However, clinical practice showed that SIRS-criteria were characterized by low specificity against the background of high sensitivity and often failed to distinguish a physiological inflammatory reaction from a dysregulated, pathological response. Accordingly, its prognostic value was significantly limited.
Sepsis-3
In 2016, as a result of the third international consensus, the understanding of sepsis fundamentally changed. By the new definition, sepsis is considered as a life-threatening organic dysfunction caused by the organism’s dysregulated response to infection.
Within the framework of this concept, septic shock was formed as a subgroup of sepsis, during which circulatory and metabolic disturbances sharply increase the risk of lethality. While the diagnostic criteria of shock were determined as follows:
The necessity of vasopressors to maintain the mean arterial pressure (MAP) at a mark of ≥65 mm Hg;
Serum lactate level >2 mmol/L despite adequate fluid resuscitation (infusion therapy).
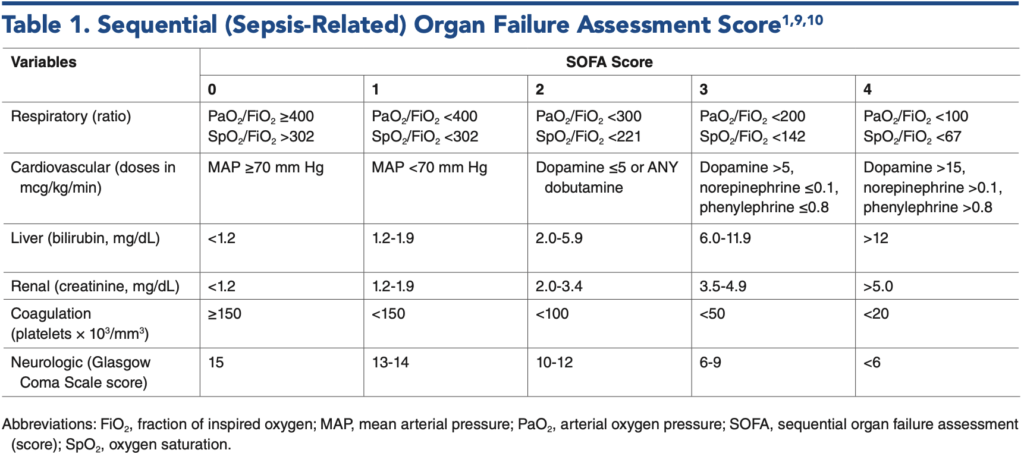
During this same period, the SOFA scale was introduced for the objective evaluation of the degree of organic failure. The mentioned system analyzes the functional state of six main organic systems (respiratory, coagulative, hepatic, cardiovascular, central nervous, and renal). An increase in points by ≥2 is clinically important, because it is directly connected to a high probability of mortality.
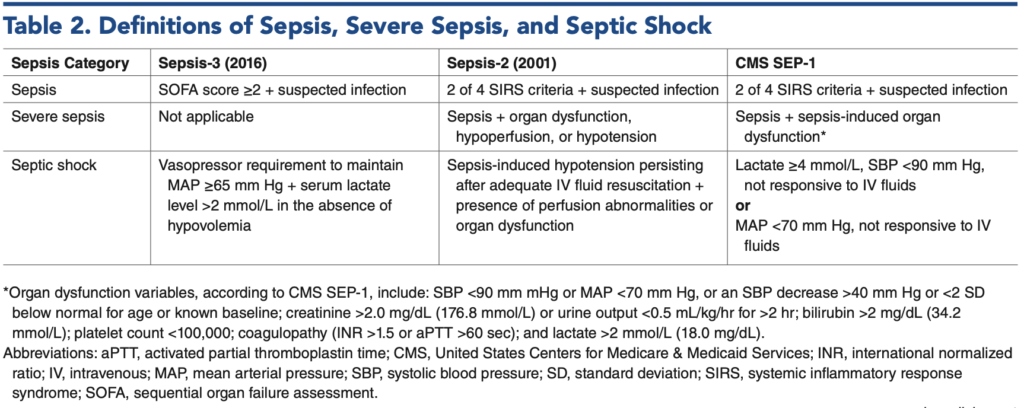
CMS SEP-1 Inconsistency
Despite the introduction of Sepsis-3, the federal regulatory standard (CMS SEP-1) still maintains a retrospective approach. To this day, it relies on the term “severe sepsis” (infection + organic dysfunction or lactate >2 mmol/L). For the verification of septic shock, a sufficient criterion for CMS represents a systolic blood pressure (SBP) <90 mm Hg or a lactate indicator ≥4 mmol/L, without the necessity of using vasopressors. This obvious inconsistency existing between definitions determines a significant bureaucratic and medicinal disparity in clinical practice.
Sepsis Screening
A unified consensus on a universal instrument for sepsis screening still does not exist in the medical community. Significant differences are noted in terms of diagnostic accuracy among the methods established in clinical practice:
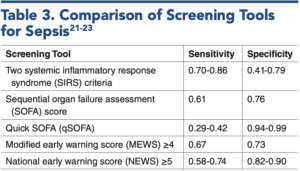
SIRS: Characterized by high sensitivity, although due to low specificity it often determines “false positive” results.
qSOFA: Its sensitivity fluctuates between 48%−72%, while its specificity reaches 72%−85%. Due to low sensitivity, the 2021 Surviving Sepsis Campaign guideline removed the recommendation on its use as a primary screening instrument.
NEWS and MEWS: Represent integrated scales of vital functions. They possess an average level of prognostic value and are characterized by diagnostic limitations similar to other methods.
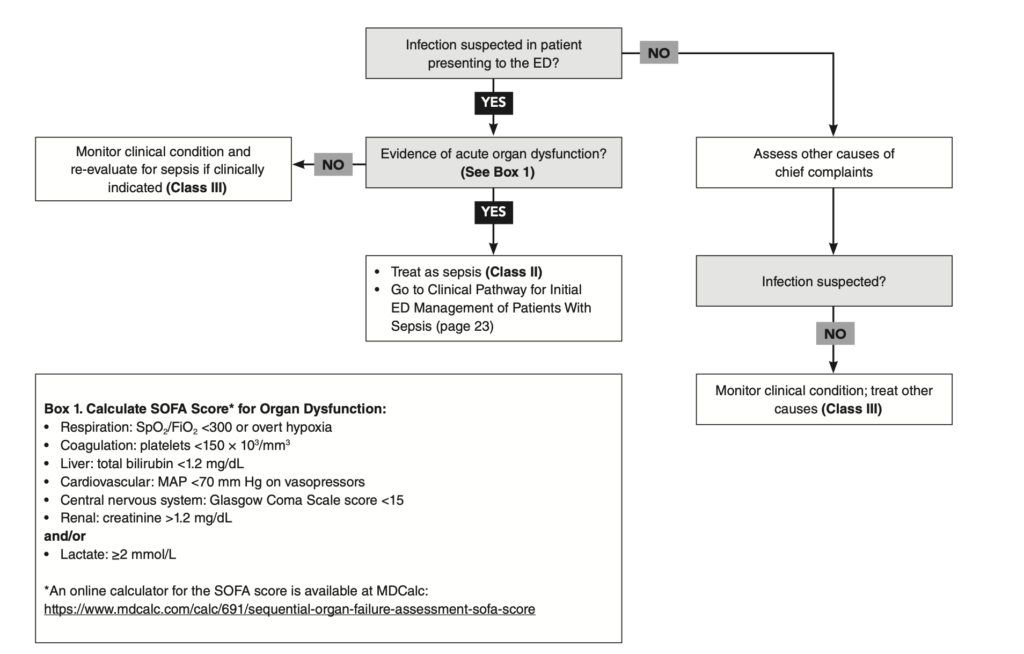
It should be emphasized that organic dysfunction revealed against the background of a suspected infection or a lactate indicator >2 mmol/L is an unconditional indicator for an in-depth clinical-laboratory evaluation of sepsis, regardless of the primary results of screening tests.
The Practical Value of the SOFA Scale
Despite the fact that the SOFA scale is considered as the “gold standard” for predicting the outcome of the disease, its routine use in emergency help departments is connected to certain difficulties. This is caused by the fact that such components of the scale as the analysis of arterial blood gases () and the serum bilirubin level require specialized laboratory research.
In acute clinical situations, the mentioned data are not always immediately accessible, because of which in practice they often turn to modified versions of SOFA.
The Role of Artificial Intelligence
At the modern stage, machine learning models appear as an important helper in the process of making clinical decisions, especially during atypical clinical manifestations of sepsis. For example, the validation of the Epic Sepsis Model (ESM) showed that the introduction of the algorithm reduced hospital lethality by 44% (sensitivity – 86%, specificity – 81%).
However, “Alert Fatigue” represents a technological challenge. Due to excessive and often non-specific signals, desensitization of medical personnel occurs, which hinders timely reaction to real clinical threats. Precisely because of this, the goal of future algorithms is the optimization of the notification system and the improvement of screening accuracy.
Management of Sepsis in the Emergency Department
Initial Assessment of the Patient
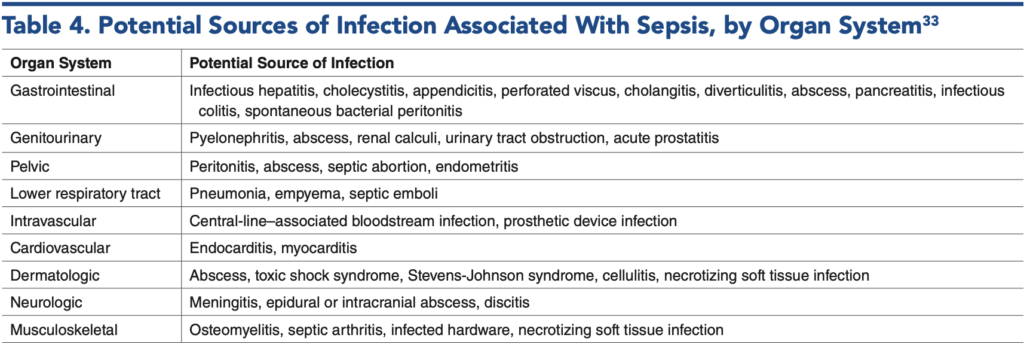
In case of suspicion of sepsis, collecting a targeted anamnesis gains critical importance, because it establishes the probable focus of infection and the modifiers of resuscitation measures. Priority attention must be paid to such infectious risk factors as recent hospitalization, surgical interventions, a course of antibiotic therapy, and an immunocompromised state. In parallel, it is necessary to evaluate the exposure environment, which includes the existence of invasive devices (catheters, implants), the use of intravenous drugs, and the patient’s social environment.
During a systematic clinical review, focus is made on fever, change of mental status, respiratory distress, and abdominal or urogenital symptomatology. At the same time, taking into account the medicinal anamnesis is decisive, which might cause the masking of the clinical picture. Specifically, the intake of beta-blockers and calcium channel antagonists might hinder the revelation of tachycardia (one of the early compensatory signs of sepsis), which significantly hinders timely diagnostics and the start of adequate therapy.
At the initial stage of physical examination, the evaluation of the status of the airways, breathing, and circulation (ABC) is an unconditional priority, which must precede a full clinical research. Such critical indicators as hypoxia, hypotension, disturbance of thermoregulation (hypo/hyperthermia), or hypoglycemia require immediate therapeutic intervention. Special clinical vigilance is necessary with elderly patients or patients having diabetes mellitus, because in them infectious processes of the abdominal cavity, pelvis, or perineum area often proceed covertly. Precisely because of this, source control remains a fundamental aspect of sepsis management.
In parallel, for the purpose of maximum increase of diagnostic accuracy, taking blood cultures is necessary. The removal of infected catheters must occur as soon as alternative vascular access is ensured, which facilitates the elimination of the source of bacteremia and hemodynamic stabilization.
Diagnostic Algorithm and Biomarkers
The diagnostics of sepsis is based on the integration of mandatory and selective research. The basic panel includes a general blood analysis, a metabolic profile (to assess kidney function and acid-base balance), serum lactate, and double blood culture before starting antibiotic therapy. Additional tests (blood gases, functional liver tests, procalcitonin) are prescribed according to clinical indication. Among visualization research, computed tomography (CT) is leading, which changes management tactics in 85.5% of cases, while ultrasound research (POCUS) increases diagnostic sensitivity by an additional 25%.
During the evaluation of hypoperfusion, initial lactate (>2 mmol/L) is a most important marker, although the 24-hour clearance of lactate is a far more reliable prognostic indicator of 90-day lethality. While the ANDROMEDA-SHOCK study confirmed that the normalization of capillary refill time is as effective for hemodynamic monitoring as the control of a 20% lactate clearance every two hours.
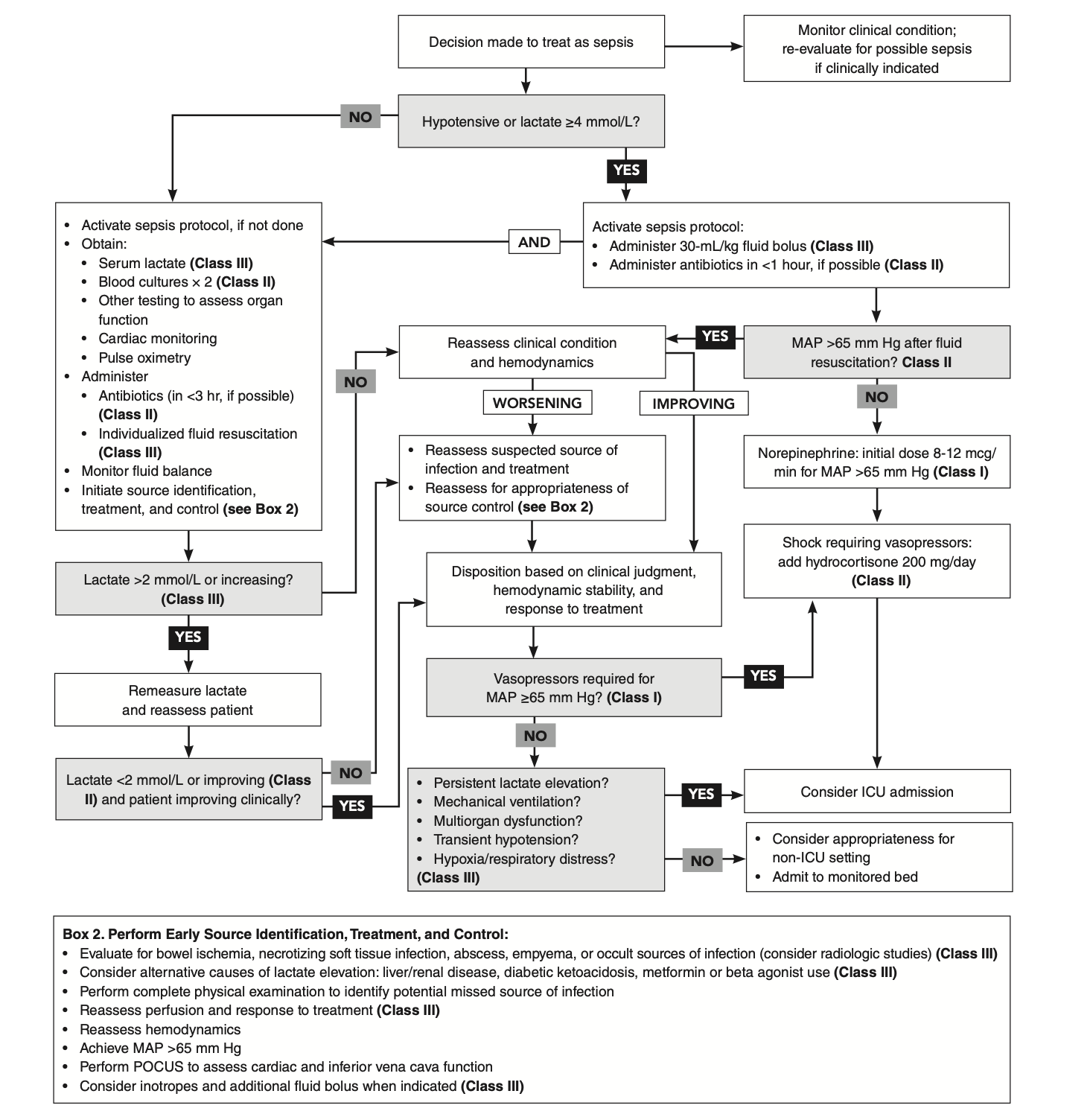
Resuscitation Bundles
Sepsis management is oriented on standardized resuscitation bundles. The universal 3-hour interval includes the determination of lactate, taking blood cultures, broad-spectrum antibiotic therapy (in case of high risk—within 1 hour), and the infusion of isotonic crystalloids (30 mL/kg) during hypotension or hyperlactatemia (>4 mmol/L).
During persistent hypoperfusion, a 6-hour protocol is activated, which implies the repeated control of lactate, the use of vasopressors (MAP ≥65 mm Hg), and the re-evaluation of the perfusion status. It is noteworthy that CMS considers as permissible the correction of the infusion volume taking into account the patient’s individual clinical state (e.g., heart failure, obesity), on the basis of corresponding documentation.
Infusion Therapy in Sepsis
Determining the optimal volume of fluid in sepsis management is still a subject of debate. Large-scale randomized studies (CLOVERS and CLASSIC) showed that between “liberal” (aggressive infusion) and “restrictive” (early use of vasopressors) strategies following the initial bolus, the lethality indicator is identical. A meta-analysis of 13 clinical studies also confirmed that neither approach possesses an advantage in terms of the prevention of side effects. Accordingly, effective guidelines remain conservative: in the absence of contraindications, the use of 30 mL/kg of balanced crystalloids is recommended at the initial stage.
Composition of Solutions and Monitoring of Hemodynamic Response
During infusion therapy, the qualitative composition of the solution is as much a priority as its volume. Large-scale studies (SMART and SALT-ED) highlighted the sharp advantage of balanced crystalloids (Ringer’s lactate, Plasma-Lyte) compared to 0.9% physiological solution (NaCl). Their use reduces the risk of acute kidney damage, the necessity of replacement therapy, and lethality by 10−15%.
For evaluating the volemic status, modern medicine assigns priority to dynamic methods, which determine in real time the response of the cardiac output to fluid:
Passive leg raise: Is a non-invasive simulation of volume loading, which ensures the mobilization of blood from venous reservoirs toward the heart.
Ultrasound research of the inferior vena cava (IVC): Is characterized by high specificity (86%), although while interpreting data, the influence of intra-abdominal pressure should be taken into account.
Current recommendations urge clinicians to maximally restrict the use of such static indicators as central venous pressure (CVP) or PAWP, because they possess a low validity for adequately predicting the response to fluid.
Antimicrobial Therapy: Timeliness, Empirical Selection, and Rational Management
In sepsis management, starting antibiotic therapy in a timely manner is a decisive prognostic factor. According to the Surviving Sepsis 2021 guideline, the urgency of intervention is determined by the patient’s clinical status:
Confirmed sepsis or septic shock: Requires the administration of antibiotics during the very first hour from identification (“Golden Hour”).
Possible sepsis without shock: If the patient is stable, a 3-hour diagnostic interval is permissible to specify the clinical picture.
Low probability of infection: Active monitoring is recommended for the prevention of inadequate use of antimicrobial preparations.
A large-scale retrospective analysis (166,559 patients) confirmed the validity of this stratified approach, especially during septic shock, where early therapy is directly connected to a reduction in lethality.
Principles of Empirical Therapy
Before identifying the causative agent, the selection of an empirical scheme is based on the probable focus of infection, local resistance, and the patient’s anamnesis. The standards of management of the main clinical scenarios are:
Pneumonia: Combination of ceftriaxone (2 g) and vancomycin (15−20 mg/kg).
Urogenital infections: Ceftriaxone (if necessary—associated with vancomycin).
Abdominal infections: Piperacillin-tazobactam or carbapenems.
Meningitis: Ceftriaxone (2 g), vancomycin, and dexamethasone.
Necrotizing fasciitis: Aggressive combination of vancomycin, piperacillin-tazobactam, and clindamycin.
In the existence of multi-resistant strains (e.g., ESBL) in the anamnesis, modifying the scheme by including preparations against extended-spectrum beta-lactamase is necessary.
Selection of Vasopressors, Administration, and Supportive Therapy
For hemodynamic stabilization during septic shock, the first-line drug of choice is noradrenaline. Its infusion begins with an initial dose of 0.05 μg/kg/min and continues with subsequent titration until achieving the target indicator of mean arterial pressure (MAP ≥65 mm Hg). The advantage of noradrenaline is determined by a pronounced alpha-adrenergic effect, which ensures the restoration of vascular tone. Until ensuring central venous access, the introduction of the preparation from a peripheral vein is considered safe during the first 6 hours.
Second-line Preparations and Additional Agents
In the case where the use of noradrenaline does not give a sufficient result, second-line agents are involved in the therapy:
Vasopressin (0.03 units/min): Is prescribed for the optimization of the noradrenaline dose and pressure stabilization.
Adrenaline (epinephrine): Is considered as a combined inotropic and vasopressor means during severe shock.
Dobutamine (2−20 μg/kg/min): Is used for improving perfusion during low cardiac output, although it requires monitoring due to possible iatrogenic hypotension.
By modern recommendations, due to the high risk of arrhythmias and the increase in lethality, the use of dopamine and phenylephrine during sepsis is not expedient.
Hybrid Resuscitation and Corticosteroids
The modern standard, which is known by the name of “hybrid resuscitation,” implies the parallel use of infusion therapy and peripheral vasopressors in decompensated patients. The mentioned strategy aims at the rapid optimization of hemodynamics and the timely restoration of the perfusion of vital organs.
As supportive therapy, hydrocortisone (200 mg/day) is recommended during vasopressor-dependent septic shock. The preparation effectively reduces the duration of shock, and in cases of severe pneumonia—the lethality indicator and the necessity of mechanical ventilation.
Management of Vasoplegia
Resistant vasoplegia represents a critical challenge in sepsis management, when traditional catecholamines can no longer ensure the maintenance of adequate vascular tone. In such cases, alternative, “rescue” therapeutic approaches come to the fore:
Methylene blue: Its action is based on the inhibition of nitric oxide synthases (iNOS/eNOS), which restores vascular reactivity independently of catecholamines. Randomized studies and a meta-analysis (n=556) confirmed that methylene blue reduces the duration of dependence on vasopressors and the lethality indicator during resistant shock.
Hydroxocobalamin: The mechanism of action of the preparation is connected to the binding of hydrogen sulfide () and the reversibility of vascular collapse. Primary clinical observations revealed a sharp reduction in the necessity of vasopressors, although the completion of large-scale studies is necessary for the full validity of the method.
Peculiarities of Sepsis Management in Specific Populations
The clinical management of sepsis requires special caution in those groups of patients where the physiological state changes the standard symptomatology and therapeutic response:
Elderly patients: A chronic inflammatory background and decreased immune reserve determine the aggressive course of sepsis and the high probability of an unfavorable outcome.
Persons having cirrhosis and end-stage renal disease (ESRD): Despite basic hemodynamic anomalies, infusion resuscitation is a priority, although it requires strict personalization and accuracy of volume loading.
Pregnant women: Gestational physiological changes often mask the classical signs of sepsis, which delays verification and increases the risk of perinatal complications.
Criteria for Hospitalization and Prognostic Markers
Absolute indication for the patient’s hospitalization in the intensive care unit (ICU) is the necessity of mechanical ventilation, vasopressor support, and multi-organ dysfunction. Hyperlactatemia (≥4 mmol/L) and persistent hypotension are considered as primary prognostic markers of the progression of the condition.
Risk Management and Common Clinical Errors
Errors committed in the process of sepsis management might cause a fatal result. Most often, the following flaws are encountered in practice:
Focusing only on small, obvious infections and ignoring the systemic picture;
Ignoring automated notifications sent by electronic medical systems;
Incomplete physical examination of the patient, because of which the focus of infection remains covert;
Premature fixation on troponin increase (which is often caused by sepsis and not by a primary cardiac pathology);
Failure of volemic status and pressure optimization until the stage of intubation.
Regulatory Challenges and Perspectives of Sepsis Management
The transition to a “Value-Based Care” funding model planned for 2026 activates the discussion in medical circles around the CMS SEP-1 protocol. The main challenge is the potential over-use of antibiotics and the strict regulation of infusion volumes. Professional unions emphasize the necessity of maintaining clinical autonomy, so that regulatory standards do not hinder therapy tailored to the patient’s individual needs.
Ultimately, the effectiveness of sepsis management goes through the practicality of evidence-based guidelines. Improving the clinical outcome depends not only on the formal execution of the protocol, but on the continuous monitoring of the patient’s status and the timely personalization of therapy. Diagnostic accuracy, an adequate infusion strategy, and the rational use of innovative methods create that foundation which gives the possibility of bringing the lethality indicator to a minimum even in conditions of resistant shock.
Source: Emergency Medicine Practice
