
The 2026 ACC/AHA guideline is a comprehensive update of the 2018 recommendations, now encompassing the entire spectrum of dyslipidemias—low-density lipoprotein (LDL-C), hypertriglyceridemia, and lipoprotein(a) (Lp(a)). The main priority of this multidisciplinary guideline is early intervention and the reduction of cardiovascular disease risk throughout the lifespan.
To this end, the document utilizes the PREVENT-ASCVD (Prevention of Atherosclerotic Cardiovascular Disease) calculator to specify risk and envisions the restoration of LDL-C and non-HDL-C target indicators. The guideline advocates for the broad use of biomarkers (apoB and Lp(a)) and the expansion of indications for non-statin therapy based on the latest clinical trials (CVOTs).
Special attention is paid to specific populations and strategies for overcoming therapeutic “inertia.” The document’s structure prioritizes risk discussion between the doctor and the patient, lifestyle optimization, and the implementation of personalized pharmacotherapy according to absolute risk.
Definitions and Classifications
Definitions of Dyslipidemia
The guideline establishes standardized definitions of dyslipidemias that are directly and causally linked to atherosclerotic cardiovascular disease (ASCVD). Elevated LDL-C is defined as mg/dL (3.4 mmol/L) in the general population, while in high-risk individuals, this threshold decreases to mg/dL (2.6 mmol/L). If the indicator reaches or exceeds mg/dL (4.9 mmol/L), it points to severe hypercholesterolemia, which is often caused by a familial form of the disease.
Another solid marker is Non-HDL-C (total cholesterol minus HDL-C). A level of mg/dL (3.4 mmol/L) indicates high risk, which is particularly noteworthy during triglycerides (TG) within the 150-499 mg/dL range. Under these conditions, the exact number of atherogenic particles is best reflected by ApoB ( mg/dL or 1.3 g/L).
Regarding hypertriglyceridemia, it is divided into three categories: moderate (150-499 mg/dL [1.7-5.6 mmol/L]), severe (500-999 mg/dL [5.6-11.2 mmol/L]), and very severe ( mg/dL [ mmol/L]). From a clinical standpoint, it is critical that the risk of developing pancreatitis increases sharply when the indicator is higher than 500 mg/dL.
Lipoprotein(a) deserves separate mention; high levels ( mg/dL or 125 nmol/L) occur in one-fifth of the population and determine a multiplicative increase in ASCVD risk. Against this background, low HDL-C (<40 mg/dL in men, <50 mg/dL in women) remains an important risk factor, though its correction is a secondary task after reaching target LDL-C levels.
ASCVD Risk Categories
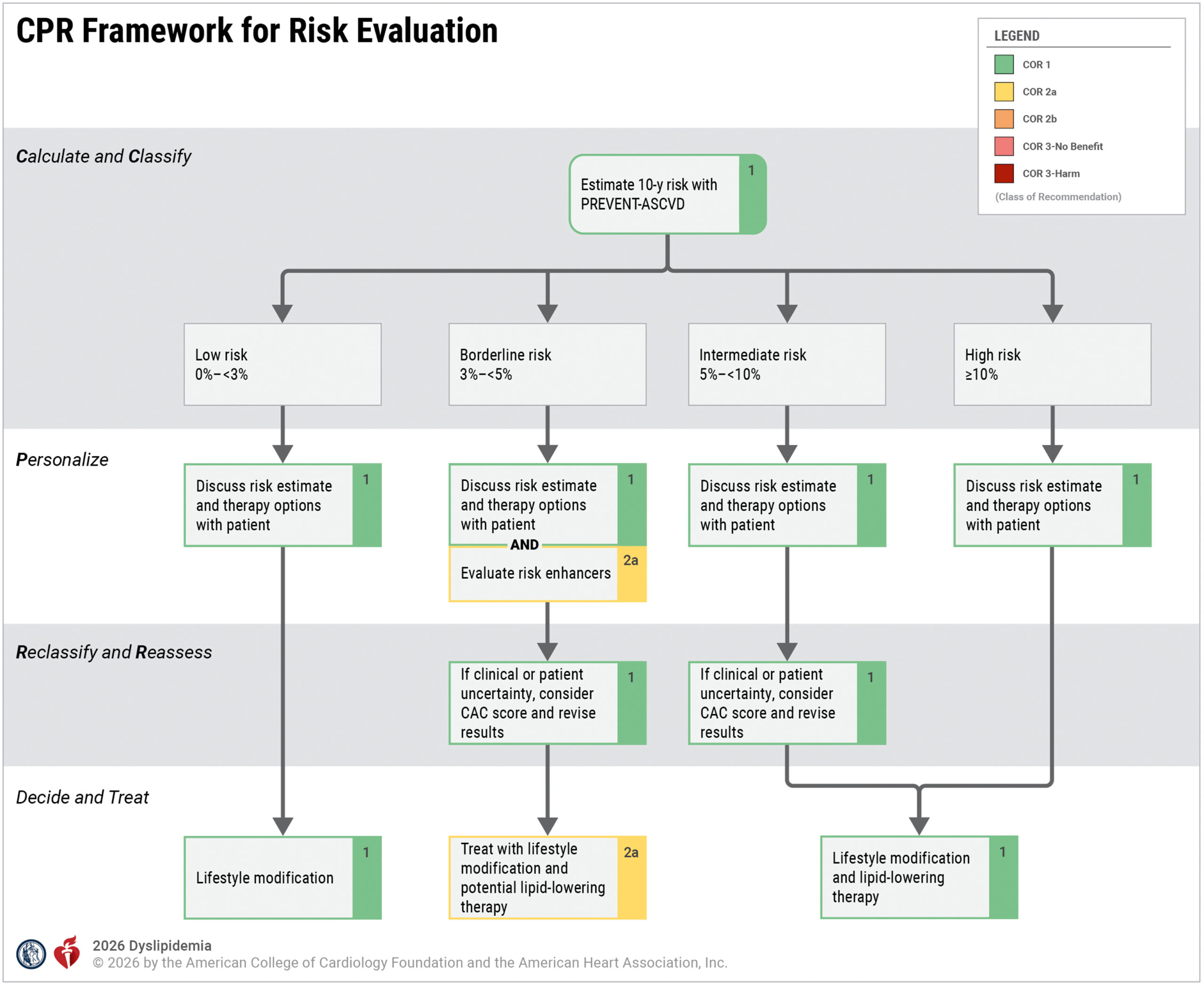
In the risk stratification process, the guideline uses PREVENT-ASCVD formulas, which allow for prediction over 10- and 30-year periods. Based on the data obtained, patients are divided into five main groups: low (<3%), borderline (3%–<5%), intermediate (5%–<7.5%), high (7.5%–<20%), and very high () risk categories.
Along with these indicators, risk-enhancing factors play a vital role in decision-making. These include a family history of premature ASCVD, metabolic syndrome, chronic inflammatory diseases, HIV infection, and elevated Lp(a)/apoB. Severe hypercholesterolemia (HeFH/HoFH) and subclinical atherosclerosis (CAC AU) require special attention, as these conditions automatically place the patient in the very high-risk category.
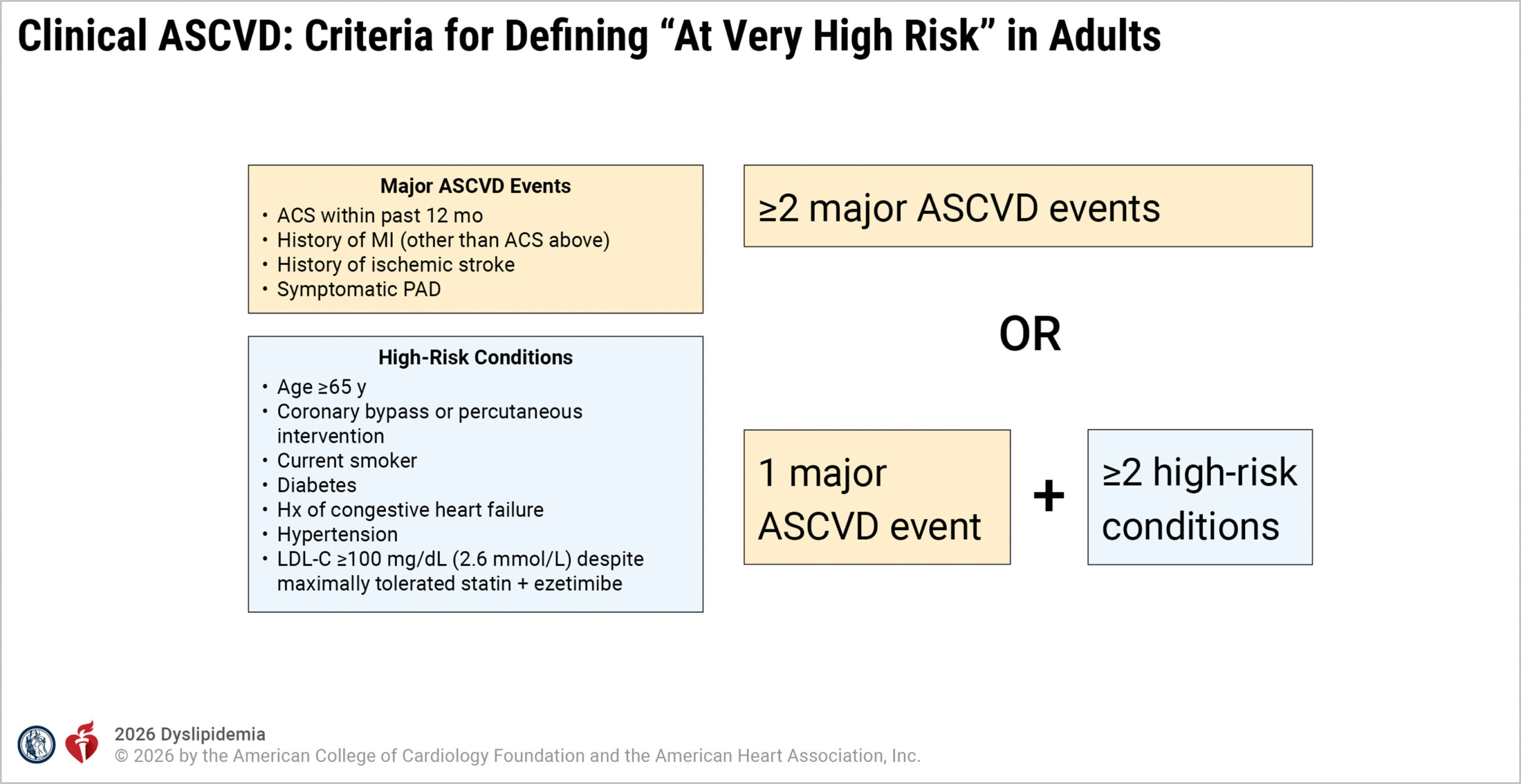
Similarly, after myocardial infarction, stroke, or revascularization, the patient belongs to the very high-risk category. This classification is a priority and is no longer dependent on initial lipid levels.
Evaluation and Diagnosis
Initial Lipid Assessment
For adults aged 20 or older, the guideline recommends a universal lipid profile determination every 4-6 years. A non-fasting panel including total cholesterol, HDL-C, triglycerides (TG), calculated LDL-C, and non-HDL-C is sufficient for primary assessment.
Testing moves to a fasting state if the postprandial triglyceride level is mg/dL. Fasting is also necessary when a genetic disorder is suspected or in children with a burdened family history.
LDL-C is determined using the Martin-Hopkins formula as long as TG concentrations remain below 400 mg/dL. If this threshold is crossed, direct laboratory determination becomes necessary. Furthermore, Non-HDL-C should be universally reflected in all laboratory reports, as it changes in parallel with apoB during hypertriglyceridemia.
Determining ApoB (COR 2a) is clinically expedient when TG levels are in the 150–499 mg/dL range and a discrepancy with LDL-C is observed. Its measurement is also a priority in diabetes mellitus or for re-evaluating the patient’s risk category. The main advantage of ApoB over non-HDL-C is a more accurate reflection of atherogenic particle count. This makes it the best clinical guide for intensifying and adjusting therapy.
According to modern guidelines, universal Lp(a) screening (COR 1) is recommended at least once in a person’s lifetime. It is desirable for the laboratory indicator to be reflected in nmol/L or mg/dL. Clinically, an indicator of nmol/L (50 mg/dL) is considered a serious risk enhancer. In such cases, much more intensive management of LDL-C and other modifiable factors (e.g., blood pressure or diabetes) is necessary. Routine repeated testing is not required and is only performed when starting PCSK9 inhibitors or lipoprotein apheresis.
Evaluation of Secondary Causes
Before starting treatment, it is critically important to screen for conditions that may secondarily cause changes in the lipid profile. Such factors include hypothyroidism, nephrotic syndrome, liver diseases, diabetes mellitus, obesity, and excessive alcohol consumption. The influence of certain medications, such as estrogens and corticosteroids, should also be considered. These causes are identified through history taking, physical examination, and targeted laboratory studies (TSH, creatinine, A1c, ALT/AST).
Lifestyle and Non-Pharmacological Management
Nutritional Interventions
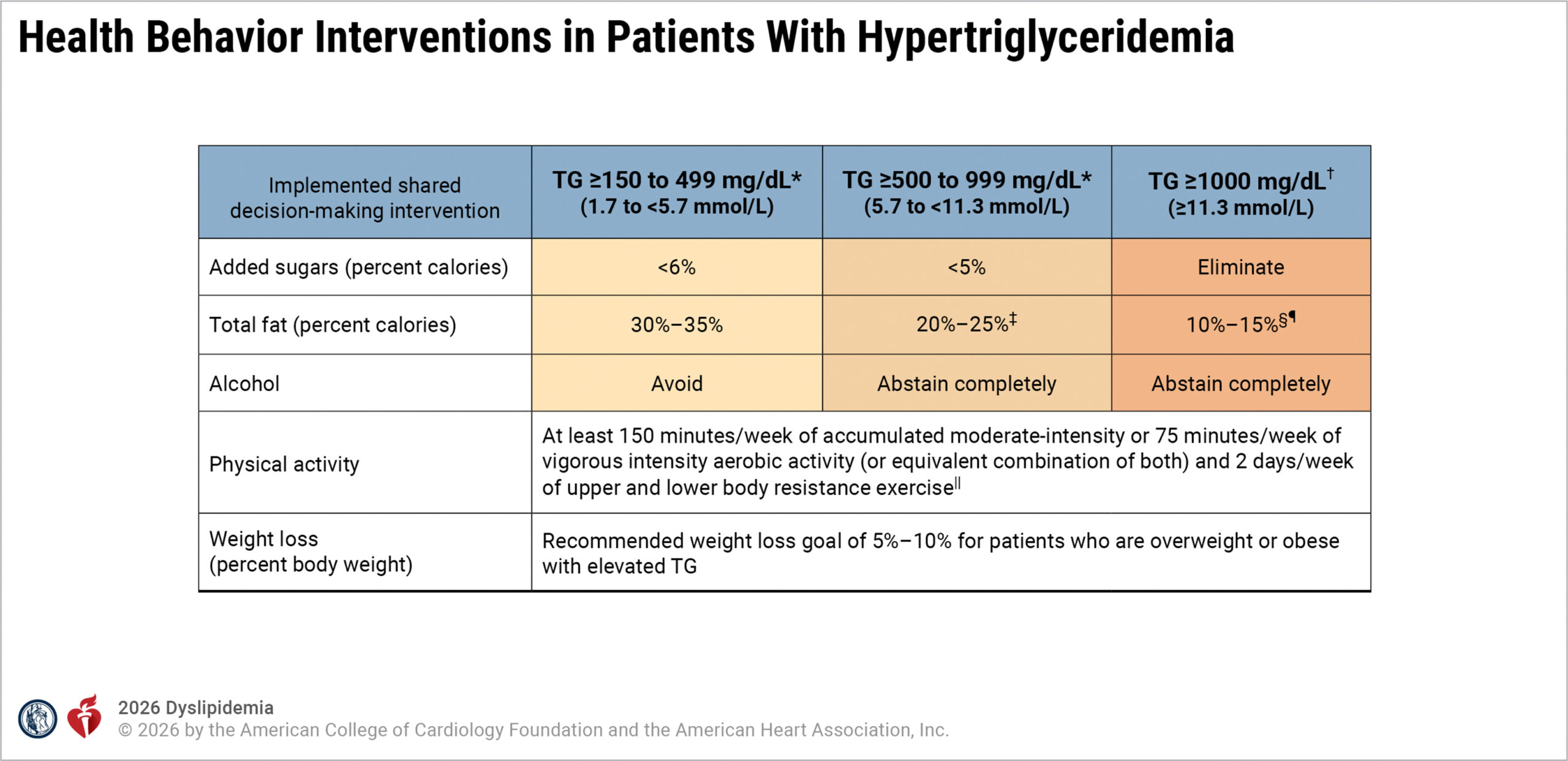
A heart-healthy diet is fundamental. This approach emphasizes vegetables, fruits, whole grains, legumes, nuts, fish, and poultry. Simultaneously, strict restriction of saturated fats (<6% of calories), trans fats, processed meats, added sugars, and refined carbohydrates is necessary. Mediterranean and DASH diets reduce LDL-C by 10-15% and triglycerides (TG) by 10-20%.
During severe hypertriglyceridemia, a special approach is needed. To prevent pancreatitis in patients with FCS, a very low-fat diet (<15% of calories from fat, <20 g/day) is used. If TG levels are mg/dL, complete removal of alcohol is mandatory.
Physical Activity
Regular aerobic exercise (150 minutes of moderate-intensity or 75 minutes of high-intensity per week) reduces TG levels by 10-20% and increases “good cholesterol” (HDL-C) by 5-10%. Aerobic load is effectively supplemented by resistance training. Additionally, weight loss has a direct link to lipids: every 1 kg reduction in body mass leads to a decrease in triglycerides by approximately 4 mg/dL.
Primary Prevention Strategies
General Primary Prevention in Adults of 30–79 Years with an LDL-C Indicator of 70–189 mg/dL (1.8–4.9 mmol/L)
The guideline establishes a strictly structured framework for primary prevention. Discussion between the doctor and the patient about risk begins when the 10-year probability of developing ASCVD reaches the ≥3% threshold. In this process, updated PREVENT formulas are used, which give much more accurate results than the predecessor PCE (Pooled Cohort Equations). The mentioned accuracy is determined by the integration of modern epidemiological data and the full exclusion of race as a biological variable.
For adults from 30 to 79 years of age whose LDL-C is within the range of 70–189 mg/dL (1.8–4.9 mmol/L), lifestyle modification represents the cornerstone of treatment. This approach envisions a healthy diet, weight control, tobacco cessation, and regular aerobic exercise (≥150 minutes of moderate or ≥75 minutes of high intensity per week). The primary re-evaluation of the patient’s condition occurs in 4-12 weeks from the intervention.
The indication for starting pharmacotherapy increases proportionally along with the increase in risk. Moderate-intensity statins (atorvastatin 10-20 mg, rosuvastatin 5-10 mg) are prescribed during borderline (3%–<5%) and moderate (5%-<7.5%) risk. At this stage, therapy aims at reducing LDL-C by ≥30% or bringing it down to a <100 mg/dL mark.
In cases of high (≥7.5%) risk, high-intensity statins (atorvastatin 40-80 mg, rosuvastatin 20-40 mg) are already used. At this time, reducing the target indicator by ≥50% or achieving the <70 mg/dL mark is necessary. While in those cases where triglycerides are within the range of 150-499 mg/dL, non-HDL-C and apoB are measured for the purpose of specifying risk.
Severe Hypercholesterolemia (HeFH and HoFH)
The guideline defines familial hypercholesterolemia strictly and accurately. The heterozygous form (HeFH) is diagnosed in adults with an LDL-C indicator of 190-400 mg/dL and by the Dutch Lipid Clinic criteria. Regarding the more severe, homozygous form (HoFH), LDL-C here exceeds 400 mg/dL, and for confirmation, Simon Broome criteria or genetic research are used.
Familial chylomicronemia syndrome (FCS) occupies a special place in the disturbances of triglyceride metabolism. It is characterized by a TG >1000 mg/dL indicator, which is caused by genetic variants of the lipoprotein lipase (LPL) pathway. In contrast to this, multifactorial chylomicronemia syndrome (MCS) is determined by both polygenic and various secondary causes.
The mentioned diagnostic accuracy represents the basis for aggressive medical intervention. In adults with HeFH, first-line treatment envisions a combination of a high-intensity statin and ezetimibe. Therapy aims at reducing LDL-C by ≥50% or achieving the <100 mg/dL mark. In case of failure to achieve the target indicator, PCSK9 inhibitors (mAbs) or inclisiran are added to the scheme.
The management of HoFH requires multimodal strengthening—the use of PCSK9 inhibitors, bempedoic acid, and lipoprotein apheresis. At this time, the main orientation of treatment is the LDL-C <70 mg/dL indicator. Along with this, the guideline gives a strict recommendation for genetic cascade screening. Special attention is also paid to youth, in whom pharmacotherapy during HeFH starts from 8-10 years of age. The mentioned approach emphasizes the decisive importance of primordial prevention.
Primary Prevention During Diabetes Mellitus
For patients from 30 to 79 years of age having diabetes mellitus, the guideline sets a strict preventive framework. The mentioned group belongs to the high-risk cohort for developing ASCVD. For them, moderate-intensity statin therapy is necessary if at least one additional risk factor is present, such as age from 40 to 75 years or albuminuria.
High-intensity therapy is prescribed in the case where the 10-year total risk amounts to ≥10%. During the process of treatment, the LDL-C <100 mg/dL and non-HDL-C <130 mg/dL indicators represent the main target orientations.
During a constant increase in the level of lipids, the strengthening of treatment occurs by the addition of ezetimibe or a PCSK9 inhibitor. Against the background of all this, lifestyle modification still remains a most important component. The mentioned approach aims at the optimization of double cardiometabolic risk and plays a decisive role in improving the patient’s outcome.
Primary Prevention During High ASCVD Risk
Persons whose 10-year total risk of developing ASCVD amounts to ≥10% require special attention. This group also includes patients with additional risk enhancers, such as a family history of premature ASCVD, metabolic syndrome, and chronic kidney disease. During the existence of such a high risk, along with the optimization of lifestyle, starting treatment with high-intensity statins represents a necessary step.
In those cases where a clinical decision requires additional accuracy, coronary artery calcium (CAC) scoring represents the best auxiliary means. This research helps the doctor in the individual specification of the level of risk. If the calcium indicator amounts to ≥100 Agatston units (AU) or ≥75th percentile, the management tactics tighten and prescribing high-intensity therapy becomes a priority.
Management of Subclinical Coronary Atherosclerosis (Men ≥40 years, Women ≥45 years)
A new section of the guideline considers coronary artery calcium (CAC) scoring and coronary computed tomographic angiography (CCTA) as decisive instruments for risk re-evaluation. The mentioned technologies serve the individual and accurate determination of the necessity of treatment. For example, when CAC ≥100 AU or ≥75th percentile, this determines the start of high-intensity statin therapy. In this case, the target of treatment is achieving the LDL-C <70 mg/dL mark.
If the calcium index is within the range of 1–99 AU, the guideline supports moderate-intensity therapy and an LDL-C <100 mg/dL target indicator. On the other hand, a zero index (CAC=0) gives the possibility of temporary deferral of pharmacotherapy. This approach concerns non-smoking persons with low risk (without diabetes mellitus) and envisions a 5-year abstinence from prescribing statins.
The mentioned strategy significantly increases the accuracy of treatment. It will avoid the unnecessary medicinal loading of those patients who do not exhibit a real risk. At the same time, this method effectively reveals the covert, initial signs of the disease in 50% of those persons who have a calcium index of more than zero.
Specific Populations
Management of Dyslipidemia During Pregnancy Planning, Pregnancy, and Lactation; Ethnic Peculiarities
Increasing maternal age, against the background of the physiological increase of lipids, significantly strengthens the risk of cardiovascular diseases (CVD). This change concerns indicators of total cholesterol (TC), triglycerides (TG), and LDL-C. Accordingly, consultation before conception serves the preliminary optimization of risk factors.
During the period of pregnancy and lactation, bile acid sequestrants (for example, colesevelam) are considered a safe means. Statins, as a rule, are contraindicated, except for cases of extreme risk (for example, HoFH). The mentioned approach serves the protection of the balance between risks of teratogenicity and data on the prevention of preeclampsia. Severe gestational hypertriglyceridemia (TG ≥500 mg/dL) requires special attention. To avoid pancreatitis, after the first trimester, the use of omega-3 fatty acids or fibrates is necessary.
During care based on ethnic belonging, the guideline assigns priority to social determinants instead of race. The mentioned approach implies a lifestyle tailored to the patient and the detailed analysis of data for various populations. This strategy increases the effectiveness of treatment taking into account the individual cultural and social environment.
Heart Failure
While managing heart failure, the role of statins is significantly dependent on the etiology of the disease. Data from clinical trials (CORONA and GISSI-HF) testify that statins do not provide benefit in the sense of reducing mortality when it concerns heart failure with reduced ejection fraction (HFrEF) of non-ischemic origin.
The final decision about continuing or starting therapy is dependent on the coexistence of ASCVD and the expected life duration of the patient. It should be taken into account that the prevalence of atherosclerotic cardiovascular disease in this population exceeds 50%. Regarding heart failure with preserved ejection fraction (HFpEF), at this stage, solid evidence regarding the effectiveness of statins is not available to us.
Chronic Inflammatory Diseases, CKD, HIV, and Cancer
During chronic inflammatory conditions (e.g. rheumatoid arthritis), standard risk calculators cannot properly evaluate cardiovascular threats. Therefore, in such patients, the strengthening of lipid-lowering therapy (LLT) occurs directly according to the activity of the disease. In the case of stage 3 or higher chronic kidney disease (CKD), at the pre-dialysis stage, the use of statins, ezetimibe, and PCSK9 inhibitors gives beneficial results. However, when starting dialysis, the effectiveness of these preparations is significantly lost. Despite this, continuing treatment that has been started is completely permissible.
Special attention is paid to HIV-infected (HIV) patients. According to the data of the REPRIEVE study, the use of pitavastatin reduces the risk of major cardiovascular events (MACE) by 35%. In this group, preference is assigned to statins having low CYP3A4 metabolism, so that undesirable drug-drug interactions are avoided.
Mortality caused by cardiovascular diseases is often increased in persons who have overcome cancer. The use of statins in this population reduces lethality caused by both general and directly oncological reasons. This therapy does not increase the risk of tumor recurrence. On the contrary, statins also significantly mitigate cardiotoxicity caused by chemotherapy.
Management of Hypertriglyceridemia
After the correction of lifestyle and optimization of statins, if the solid indicator of triglycerides (TG) amounts to ≥150 mg/dL, the re-stratification of the patient’s risk occurs. In the high-risk group (ASCVD or diabetes with an additional risk factor), when TG is within the range of 150-499 mg/dL, the use of icosapent ethyl (IPE) (4 g/day) reduces the risk of major cardiovascular events (MACE) by 25%. The mentioned result is confirmed by the REDUCE-IT study, despite the fact that certain signs of atrial fibrillation and bleeding are noted when taking the preparation.
The approach is different during sharply increased triglycerides (TG ≥500 mg/dL). In this case, the main priority represents the prevention of pancreatitis. For this purpose, fenofibrate (priority compared to gemfibrozil), prescription omega-3 fatty acids, or a very low-fat diet are used. Noteworthy is genetically confirmed familial chylomicronemia syndrome (FCS), which responds positively to a new preparation—olezarsen. While in those cases where a clinical inconsistency is observed, apoB and non-HDL-C indicators fully replace the LDL-C parameter.
Approach Toward Patients Having Elevated Lp(a)
According to the guideline, one-time testing of Lp(a) reveals 20% of those persons who have the mentioned indicator elevated (>50 mg/dL or 125 nmol/L). This condition determines a 40% higher relative risk of ASCVD. Along with this, Lp(a) together with other risk factors gives a multiplicative effect, which further worsens the patient’s condition.
In such cases, the intensive management of all other modifiable risk factors gains decisive importance. In high-risk groups, the use of PCSK9 inhibitors along with LDL-C reduces the Lp(a) indicator by 15–30%. Lipoprotein apheresis is approved by the FDA for those patients whose Lp(a) is ≥60 mg/dL and who at the same time exhibit familial hypercholesterolemia (FH) and ischemic heart (CAD) or peripheral artery disease (PAD).
It is noteworthy that new Lp(a)-specific therapies, such as small interfering RNA (siRNA) preparations, are currently in a waiting regime.
Management of Statin-Associated Muscle Symptoms (SAMS)
Statin-associated muscle symptoms (SAMS) bother approximately 10% of patients. The mentioned condition is often determined not directly by a side effect of the medication, but by the “nocebo effect.” At the initial stage of management, it is necessary to exclude secondary causes, which is represented by drug-drug interaction (DDI) or intensive physical loading.
While maintaining symptoms, a repeated trial of treatment with an alternative statin or the use of a low dose of the preparation is recommended. In those cases where taking the full dose of statin cannot be managed, ezetimibe (IMPROVE-IT), bempedoic acid (CLEAR Outcomes), or a PCSK9 inhibitor (GAUSS-3 and ODYSSEY ALTERNATIVE) is added to the therapy.
Furthermore, for those persons who have intolerance toward statins, the coronary artery calcium (CAC) indicator represents a reliable guide when selecting treatment. This research helps the doctor determine how aggressive the alternative lipid-lowering therapy should be, taking into account the individual risk.
Complications
Safety of Medications and Side Effects
In the process of lipid-lowering therapy (LLT), the issue of the safety of medications is a priority. Statins might slightly accelerate the development of prediabetes, although the benefit received in terms of the cardiovascular side significantly exceeds this risk. The mentioned preparations are completely safe even during stable liver pathologies (e.g. MASLD).
From the standpoint of laboratory control, routine checking of creatine kinase (CK) and liver enzymes, in the absence of severe clinical symptoms, does not represent a necessity. It should be noted here as well that the use of coenzyme Q10 for the purpose of reducing statin side effects is not reinforced by scientific evidence.
Medications of the non-statin group—ezetimibe, PCSK9 inhibitors, and bempedoic acid—turned out to be well-tolerated in patients. However, bempedoic acid requires specific attention. During its use, the regular monitoring of the level of creatinine, urea (BUN), and uric acid is necessary, so that metabolic complications are avoided.
Interaction of Statins and Cardiovascular Preparations
During the prescription of statins, special caution is necessary when combining them with other cardiovascular preparations. Those statins that are metabolized by the CYP3A4 enzyme (e.g. simvastatin, lovastatin) significantly increase the risk of the development of myopathy. This threat is particularly high during their simultaneous use with calcium channel blockers (CCBs) or amiodarone.
To avoid complications, preference is assigned to those statins that possess a different pathway of metabolism. Such alternative means are represented by pravastatin, rosuvastatin, or pitavastatin.
In practical activity, the timely revelation and evaluation of possible drug-drug interactions occurs according to special, detailed tables. This approach serves the selection of the most safe combination of medications for each patient.
Future Directions
Despite significant progress, certain gaps in knowledge still remain in the management of dyslipidemia, which represent the subject of future research. The mentioned spheres, first of all, include reproductive risks, inequality of healthcare accessibility, and specific changes of the lipid profile in transgender persons. The accumulation of data in this direction represents a necessary condition for the development of personalized medicine.
In the list of future priorities, first-line place should be assigned to those studies that will examine implementation strategies and the effectiveness of care managed by pharmacists. Also, special importance is assigned to the research of long-term outcomes of early lipid-lowering therapy (LLT) and surrogate markers of atherosclerotic plaque.
Furthermore, the refinement of research with CCTA and the integration of new biomarkers into clinical practice represent a sphere of scientific interest. The latter includes lipoprotein(a), polygenic risk score evaluation (PRS), and apolipoprotein B (apoB), the joint use of which will significantly increase the accuracy of predicting cardiovascular risks.
Source: JACC
