
The 2026 American Heart Association and American Stroke Association (AHA/ASA) guideline for the management of acute ischemic stroke is based on the latest evidence. The document brings the entire chain of patient management (pre-hospital stroke recognition, systemic optimization, emergency reperfusion intervention (IVT, EVT), and subsequent management) into a unified system.
Building upon the 2018-2019 recommendations, the guideline integrates the most important scientific achievements of the last decade. These studies, along with expanding the availability of reperfusion therapy, have also fundamentally changed existing treatment methods.
According to the new standards, the clinical indications for the use of endovascular therapy (EVT) are significantly increasing. It already includes patients with extensive infarct cores, pre-stroke limited capabilities, and cases of delayed hospitalization. Along with this, the document describes in detail alternative medicinal schemes for intravenous thrombolysis (IVT) and refined antiplatelet protocols. The development of primary recommendations regarding the endovascular treatment of the pediatric age group represents a special scientific value.
Pre-hospital Stage and Emergency Assistance Systems
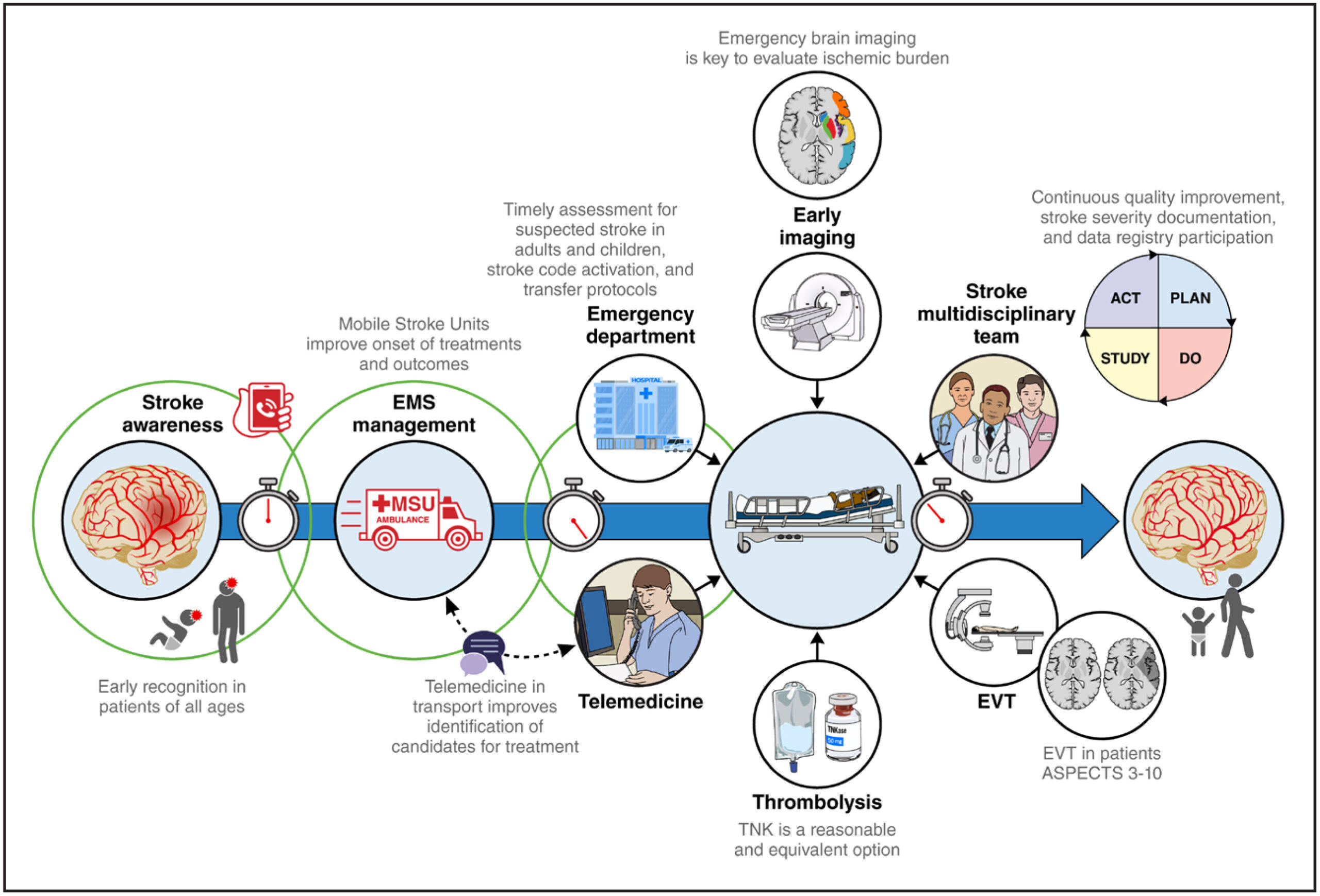
In the 2026 guideline for the management of acute stroke, the formation of organized systems of care is assigned fundamental importance. Pre-hospital triage protocols are reinforced with a Class 1 (LOE A) quality recommendation. They envision the direct transfer of patients with suspicion of a large vessel occlusion (LVO) to specialized centers. In this process, the rapid identification of LVO is critically important, for which the use of such valid scales as positive VAN, NIHSS (≥6), or RACE (≥5) is considered a priority.
Since every lost hour during a large vessel occlusion doubles the volume of the infarct, time is considered the main determinant of the therapeutic outcome. Precisely because of this, the primary task of both the direct transportation and the “Drip-and-Ship” models is to reduce the so-called DIDO time (the interval from the patient entering the first clinic until their transfer to another center) to 90 minutes.
Mobile stroke units (MSU) occupy a special place in this chain, representing specialized ambulances equipped with computed tomography (CT/CTA), a portable laboratory, and tele-medicine apparatus. Such a system gives the possibility of starting thrombolysis (administration of alteplase or tenecteplase) within the very first hour from the start of symptoms. By using MSU, a 30-40% higher rate of reperfusion and a significantly improved clinical outcome are achieved, which statistically corresponds to an mRS 0-2 mark in 55% of patients, moreover, without increasing the risk of symptomatic intracranial hemorrhage (sICH).
For the successful work of the system, it is necessary to have:
EMS personnel training: Perfect mastery of LVO scales by emergency assistance brigades.
Optimal logistics: Transfer of the patient toward high-flow thrombectomy centers (>50 procedures/year).
Strict monitoring of time: Orientation on indicators — “Door-to-Needle” (DTN <60 min) and “Door-to-Puncture” (DTP <90 min).
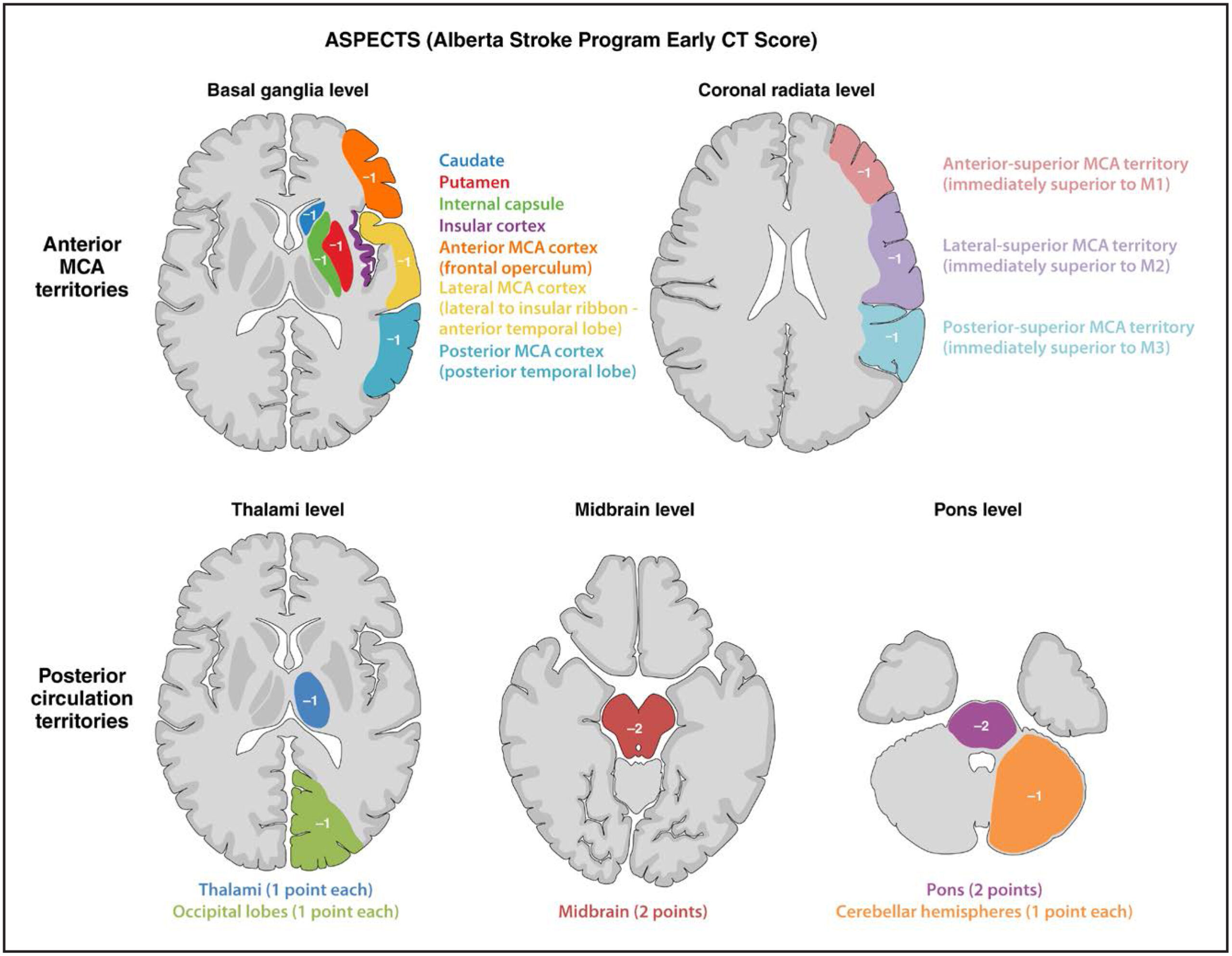
As soon as the patient enters the clinic, the priority task represents the performance of non-contrast computed tomography (NCCT) within the very first 25 minutes. The mentioned study is a necessary condition for excluding hemorrhage and for assessing the degree of brain damage by the ASPECTS scale (preferably ≥6). At the same time, the use of CT angiography (CTA) (COR 1) is considered a mandatory requirement for identifying large vessel occlusion (LVO: ICA, M1, proximal M2, basilar).
Regarding extended visualization methods, such as CT perfusion (CTP) and MRI diffusion (DWI), they are primarily used for extended time windows (4.5-24 hours) or for the selection of patients having a wide core. At this time, the volume of the infarct core (<100-150 ml), the size of the penumbra (>10 ml), and the mismatch coefficient (>1.8) are considered as selection criteria.
It is important that possible delay caused by MRI research in early windows is avoided. For this purpose, it is recommended to reconcile NCCT-ASPECTS data with CTP/DWI equivalents; for example, a hypodensity indicator of ≤26 Hounsfield units (HU) is considered a reliable prediction of tissue viability.
Parallel to the diagnostics, the management of arterial pressure before reperfusion therapy is permissible up to a mark of 185/110 mm Hg. For pressure control, the use of labetalol (10-20 mg intravenously) or nicardipine infusion (5-15 mg/h) is considered a priority in practice. After the completion of IVT/EVT procedures, to bring the risk of reperfusion hemorrhage (sICH risk 3-7%) to a minimum, the target indicator of pressure is a limit of <180/105 mm Hg.
Anterior Circulation Large Vessel Occlusion (LVO)
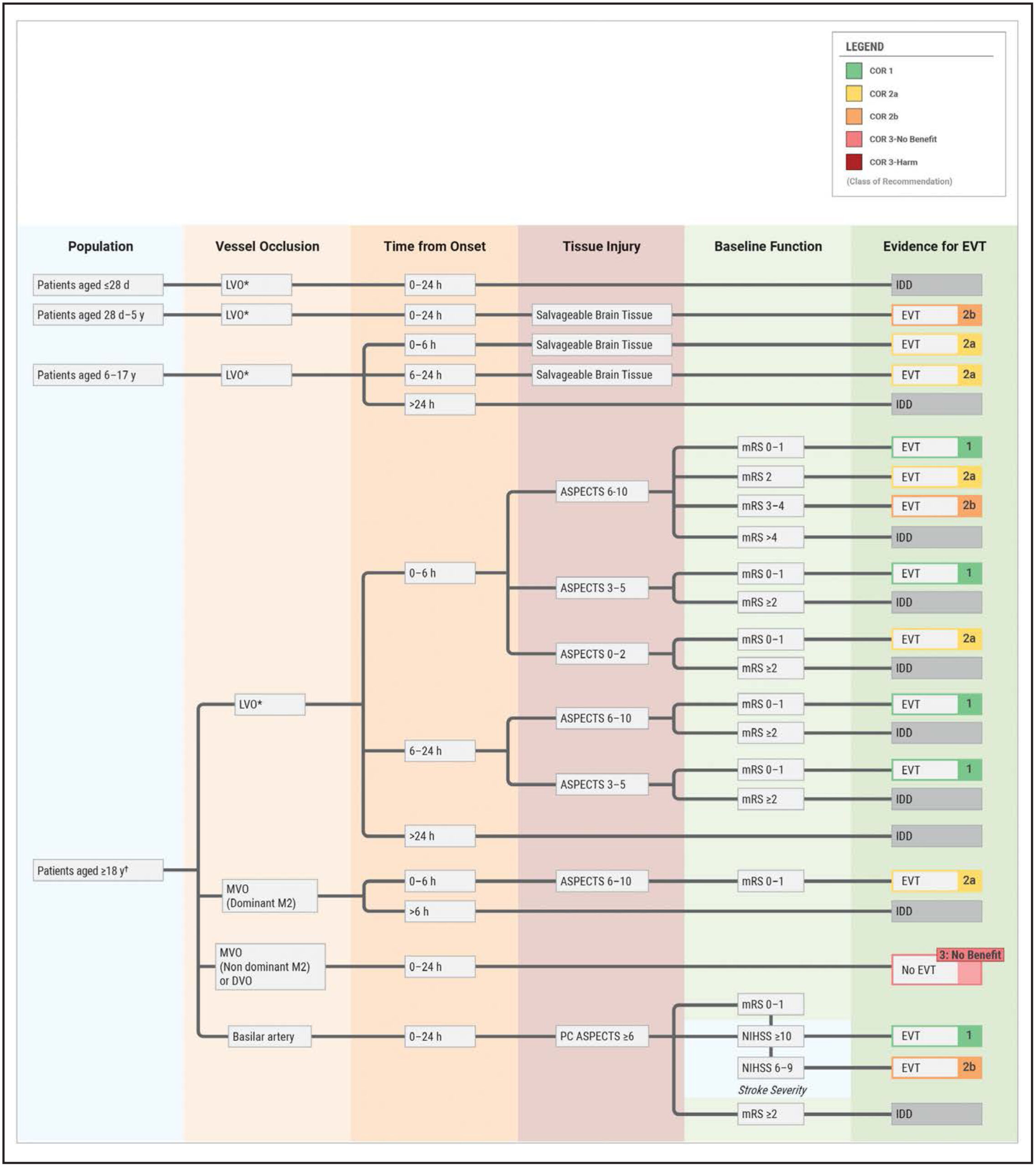
During anterior circulation LVO, which implies the blockage of the internal carotid artery (ICA) or the M1 segment of the middle cerebral artery (MCA), endovascular thrombectomy (EVT) represents a first-line (Class 1) therapy. NIHSS ≥6, pre-stroke existing mRS 0-1, and ASPECTS ≥6 (in a 0-6 hour interval) are considered as standard criteria for conducting this procedure. The mentioned time window (in accordance with DAWN and DEFUSE-3 studies) expands up to 24 hours in the existence of a perfusion mismatch, which is highly effective for the functional independence of patients (NNT 2.8-3.6).
The mentioned recommendations are based on the large-scale HERMES meta-analysis. This study confirmed that endovascular thrombectomy (EVT) is equally effective regardless of the patient’s age, time window, or previously conducted thrombolysis (IVT). At the same time, the data of COMPASS and ASTER studies give the possibility of selecting the interventional technique. Specifically, the direct aspiration method shows results similar to stent-retrievers, while during difficult, tortuous anatomy of the vessels, it is even considered a priority approach.
The most important news of the guideline concerns the management of patients having wide infarct cores. According to SELECT2 and ANGEL-ASPECTS studies, endovascular treatment (EVT) is effective even during an ASPECTS 3-5 indicator. The mentioned approach significantly increases the chance of functional independence in patients. Regarding even more extensive damages (ASPECTS 0-2), based on the LASTE study, the procedure is presented with a COR 2a recommendation. However, in such cases, it is necessary to protect strict selection criteria.
The AURORA meta-analysis conducted in the extended window (6-24 h) confirms the advantage of endovascular treatment again. It is important that pre-stroke existing disability no longer gives the basis for refusal of intervention. According to HERMES data, a significant part of mRS 3-4 patients returns to the initial state after treatment. Regarding small-caliber M2 occlusions, the performance of EVT at this time is considered individually, primarily during the damage of dominant branches or a high NIHSS (>15) indicator.
In conditions of a low ASPECTS score or pre-stroke existing limited capabilities, it is mandatory to use the principle of making a joint decision. This is necessary because in such cases the functional benefit is relatively small, while the risk of reperfusion hemorrhage and edema increases up to 5-10%. While refraining from the procedure is recommended if the patient’s expected life duration is less than 6 months, or if refractory hypertension or hypodensity >26 HU is present.
Posterior Circulation Stroke
Basilar artery occlusion requires emergency endovascular treatment (EVT, COR 1). The mentioned recommendation applies to those patients whose NIHSS ≥10 and posterior circulation ASPECTS (PC-ASPECTS) comprises an indicator of ≥6. We have a 24-hour time window from the start of symptoms for the intervention. This approach is based on fundamental studies (ATTENTION and BAOCHE), which confirmed that thrombectomy almost doubles the chance of an independent life compared to medicinal treatment.
For predicting tissue viability, the PC-ASPECTS system plays a decisive role. On this scale, 2-2 points are assigned to the pons and midbrain, and one point to each of the other segments. During intervention, the primary aspiration technique is effective, which is especially relevant during the high prevalence of intracranial atherosclerosis (~50% in Asian cohorts). Despite the fact that data on patients having a low NIHSS (6-9) indicator are still limited, a clear trend of benefit is maintained in studies.
Interventional Technique and Pediatric Recommendations
During intervention, general anesthesia and conscious sedation have an equal influence on the patient’s outcome (mRS) and the risk of complications (sICH). According to AMETIS and DIRECT-MT studies, these two methods are considered equivalents to each other. The main goal of the procedure represents the achievement of high-quality reperfusion (eTICI 2b/2c/3) and the revascularization of more than half of the vessel. Although data regarding the effectiveness of balloon guide catheters (BGC) remain contradictory, during two-level (extracranial and intracranial occlusion simultaneously) damages, emergency stenting gives significant benefit.
Regarding medicinal support, the effect of rescue stenting remains unclear until this time. At the same time, based on the data of the RESCUE-BT study, we should avoid the use of tirofiban before EVT. This is necessary because the mentioned preparation generates a high risk of hemorrhagic complications (sICH).
An important update also concerns pediatric practice. In children of 6 years and older (PedNIHSS ≥6), endovascular treatment (EVT) in specialized centers is assigned a COR 2a recommendation. According to the data of the Save ChildS Pro registry, the intervention shows sharply better results compared only to medicinal treatment. This advantage becomes especially visible during the first 6 hours from the start of symptoms.
Antiplatelet Treatment, Anticoagulants, and Other Therapeutic Approaches
For the majority of patients having non-cardioembolic ischemic stroke, after reperfusion, monotherapy with aspirin represents the drug of choice during the first 48 hours. The mentioned recommendation is based on the large-scale IST and CAST studies. These studies confirmed that the timely use of aspirin significantly reduces the risk of repeated stroke and mortality.
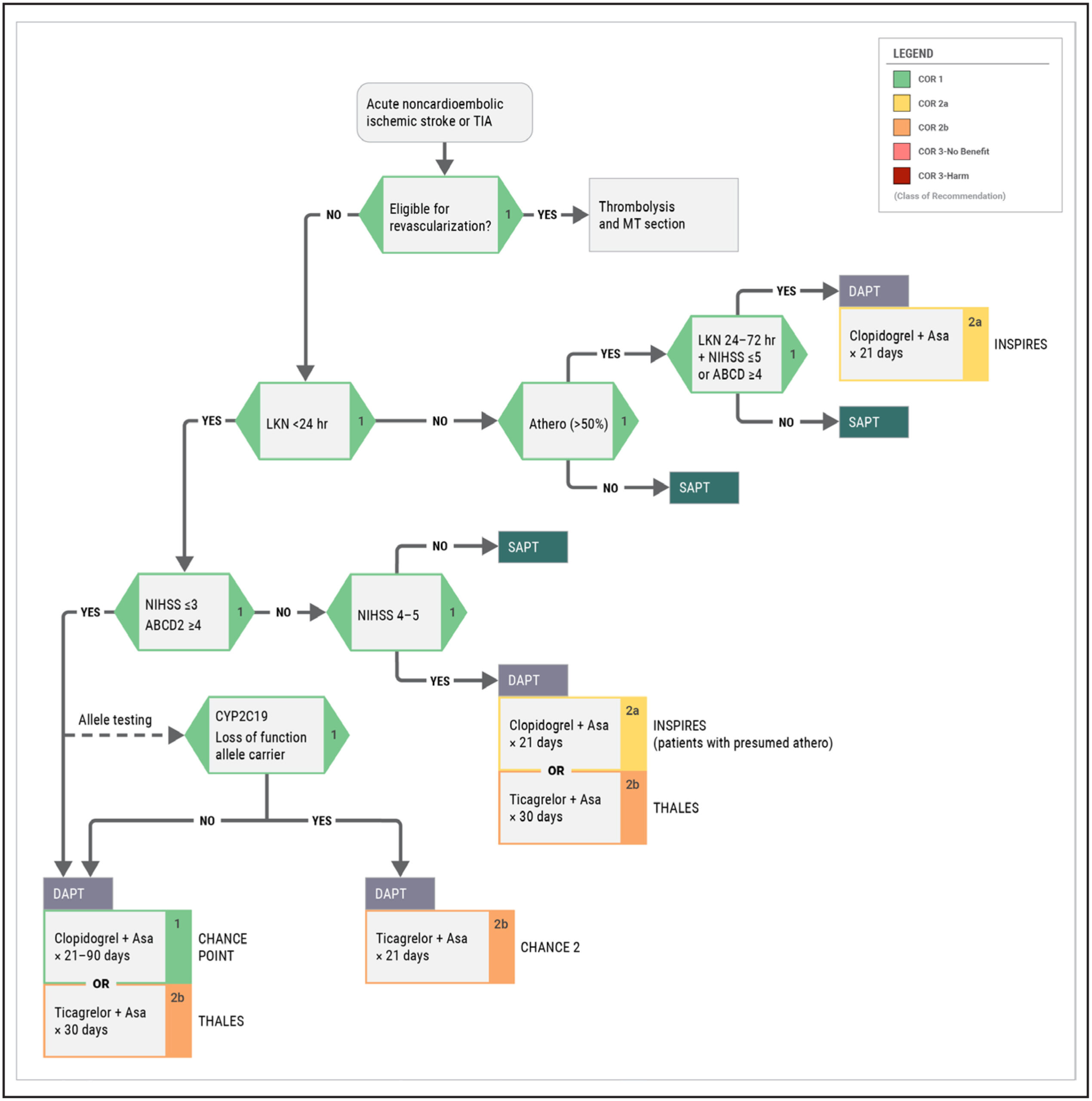
During a minor stroke (NIHSS 0-5) or high-risk transient ischemic attack (TIA), the use of dual antiplatelet therapy (DAPT) 24-72 hours after the start of symptoms is considered a priority approach. The optimal scheme of treatment implies a combination of clopidogrel and aspirin with an interval from 21 to 90 days. Studies (CHANCE, POINT, THALES) showed that such an approach significantly reduces the danger of stroke recurrence against the background of a low risk of massive hemorrhage. At the same time, due to the peculiarities of the CYP2C19 gene, preference is given to the use of ticagrelor for poor metabolizers.
However, it is necessary to show special caution in the process of treatment. We should avoid the use of antiplatelets, glycoprotein IIb/IIIa inhibitors, and triple therapy in the early stage following thrombolysis (IVT). According to the data of the TARDIS study, such an aggressive approach is harmful for the patient.
Regarding anticoagulants, their use in the acute phase of the disease has no confirmed benefit. However, during atrial fibrillation, in the case of light or medium-severity AIS, according to the ELAN study, starting direct oral anticoagulants (DOACs) is recommended within the very first 24-48 hours. It should also be noted here that the guideline does not support routine hemodilution, vasodilators, and neuroprotectors. Also, the performance of emergency carotid endarterectomy during the first 48 hours significantly worsens the clinical outcome.
Hospital Management: General Supportive Care
Stroke Units
The placement of a patient in specialized, multidisciplinary stroke units (Stroke Units) represents a recommendation of the highest priority (Class 1). Such units are characterized by 24/7 supervision of medical personnel and the involvement of physiotherapists, speech therapists, or occupational therapists. The mentioned approach reduces mortality and the degree of patient dependence on others by 20-30%.
The high effectiveness of stroke units is based on management by strictly determined protocols. This process implies the constant control of glycemia and arterial pressure, early mobilization of the patient, and the prevention of deep vein thrombosis.
Dysphagia Screening and Management
Mandatory screening for swallowing disturbance (dysphagia) is necessary during the first 4 hours after hospitalization. According to observational data, this procedure prevents cases of aspiration pneumonia by 50-70%. In case of failing the screening, the intake of food or liquid from the oral cavity for the patient is fully prohibited. This restriction remains in force until the completion of a formal assessment by a speech therapist.
During severe dysphagia, pharyngeal electrical stimulation (PES — three 10-minute sessions per day via a nasogastric tube) significantly reduces the severity of pneumonia, the risk of aspiration, the time of stay in the hospital, and dependence on tracheostomy. The mentioned effect is achieved by strengthening the activation of the corresponding areas of the brain.
Feeding and Metabolic Support
Inadequate feeding existing before a stroke significantly increases the risk of the worsening of the patient’s condition. Therefore, it is necessary to conduct screening of the nutritional status during the first 24 hours of hospitalization. The use of special valid instruments (MNA, MUST, etc.) in this process is considered a priority approach.
In patients dependent on a tube due to swallowing disturbance, starting early enteral feeding significantly reduces mortality. It is noteworthy that at the initial stage of treatment, the use of a nasogastric (NG) tube is considered more expedient compared to percutaneous endoscopic gastrostomy (PEG).
Deep Vein Thrombosis (DVT) Prophylaxis
Immobilization following a stroke creates a danger of the development of deep vein thrombosis. To avoid this complication, the use of intermittent pneumatic compression (IPC) devices is a first-line recommendation. According to the data of the CLOTS3 study, the use of these apparatuses significantly reduces the indicator of thrombosis.
Pharmacological prophylaxis with low-molecular-weight heparins is an effective means for the prevention of thromboembolism. However, it should be taken into account that such therapy increases the risk of intracranial hemorrhage to a certain extent. It should also be noted here that the guideline does not support the use of elastic compression stockings. Studies confirmed that they create a danger of skin damage/ulceration.
Post-stroke Depression (PSD)
Post-stroke depression (PSD) is noted in almost one-third of patients. For the timely diagnostics of this condition, the use of the PHQ-9 scale is considered best practice. Despite the fact that medicinal treatment (SSRIs) significantly improves the emotional background, the role of non-pharmacological methods still remains high. For example, the combined use of transcranial magnetic stimulation (rTMS) and acupuncture shows results equivalent to or better than standard therapy.
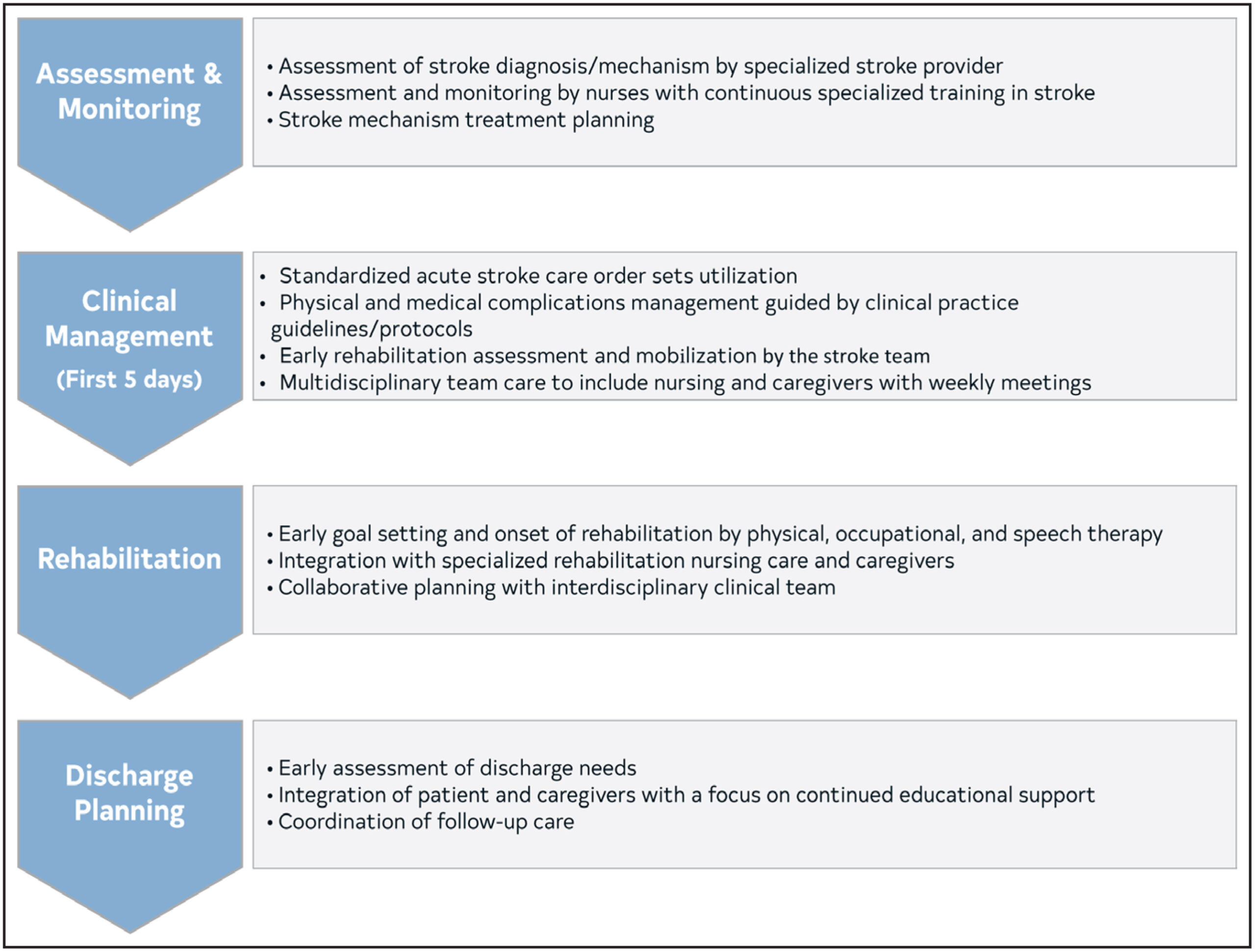
Rehabilitation
After a stroke, it is necessary to start the process of interdisciplinary rehabilitation during the first 3 days. This approach serves the restoration of the patient’s daily activities and the achievement of functional independence. However, special caution is necessary when selecting the terms of mobilization.
We must categorically avoid very early and intensive physical loading in the first 24 hours from the start of symptoms. The AVERT study confirmed that aggressive mobilization started on the very first day increases the mortality trend and worsens the 90-day clinical outcome. Accordingly, priority is assigned to standard care and starting mobilization only after 24 hours have passed.
Management of Acute Complications
Brain Edema and Surgical Intervention
Extensive infarcts are often complicated by malignant edema, which requires neurocritical supervision of the patient. Before operative intervention, conducting osmotic therapy with mannitol or hypertonic solution for the control of intracranial pressure represents a necessary condition. During extensive infarct of the middle cerebral artery (MCA), decompressive hemicraniectomy and duraplasty are recommended during the first 48 hours.
In patients under 60 years of age, the mentioned operation reduces the mortality indicator by 50%. Regarding persons older than 60 years, in their case, the benefit of intervention is primarily expressed in increasing the survival indicator and is reflected less on functional restoration.
Cerebellar Infarct
Cerebellar edema might cause compression of the fourth ventricle and acute hydrocephalus. In such cases, the performance of ventriculostomy represents an effective first-line therapy. If the patient’s clinical state still worsens, for the purpose of decompression, the performance of suboccipital craniectomy is necessary.
Seizures
Post-stroke seizures significantly increase the patient’s risk of mortality. Treatment with anticonvulsants must start as soon as the first unprovoked episode is recorded. However, it should be taken into account that the guideline does not support their routine prophylactic use.
Future Perspectives
Despite the progress achieved, many more challenges are encountered in the management of stroke. Future research envisions the refinement of the accuracy of visualization in patients having a wide infarct core and the study of the effectiveness of endovascular treatment (EVT). Special attention will be devoted to those people (mRS 3-4) and the pediatric population who already exhibited certain limitations before the stroke.
The guideline aims at the perfect equipping of stroke management teams for the practice of 2026. The main strategy includes several decisive directions: first of all, expanding the boundaries of reperfusion therapy implies increasing accessibility for those patients who until now remained outside of treatment. At the same time, the introduction of strict clinical algorithms from the pre-hospital stage until rehabilitation and protocolized management is necessary. Ultimately, the entire effort is oriented on the result, which implies the maximum reduction of disability indicators and the improvement of the patient’s quality of life.
You can find the full guidelines at the following link: AHA|ASA Journals
